PPS PRESIDENT WELCOME LETTER
It is my great pleasure to welcome you to the Pulmonary Pathology Society!
For over 30 years, the PPS has been dedicated to promoting the study and research of thoracic pathology within our medical and scientific community. The Society remains actively engaged in this mission through its educational website, its annual PPS Companion Meetings held at the United States and Canadian Academy of Pathology, and our three‑day Biennial Conferences. Beyond our formal educational activities, many of our members, past and present, continue to shape the development of research across pulmonary, pleural, and mediastinal pathology. We warmly welcome new members to join us in contributing to the future of thoracic pathology.
It is an honour to serve as PPS President for the 2026–2028 term, together with the wonderful team of Dr Anja Roden, Vice President; Dr Sabina Berezowska, Treasurer; and Dr Jennifer Boland Froemming, Secretary. My continued gratitude is extended to these friends and colleagues for their dedication and service to the Society. A special thank you is also deserved for the ongoing contributions of our webmaster, Dr Don Guinee.
We recently enjoyed an outstanding Biennial Meeting in Quebec City, a testament to the combined work of Dr Lynette Sholl, Immediate Past President, who—alongside Natasha Rekhtman, Program Committee Chair; Susan Armstrong, Program Coordinator; and Marie‑Pier Montminy, Local Organizing Chair—delivered an exceptional experience. Dr William Travis, a founding father of our Society, was duly recognised by the Awards Committee with its highest honour, the Lifetime Achievement Award. Congratulations, Bill!
We very much look forward to our next Biennial Meeting in Europe. This will be held at the Festival Hall, Lake Bled, Slovenia, between June 15–17, 2028, and will be graciously hosted by Dr Izidor Kern. Drs Yin (Rex) Hung and Jan van der Thüsen have kindly agreed to serve as Program Committee Co‑Chairs for this term, with commitments to engage widely with our many internationally allied thoracic societies to establish the very best educational programme for this conference. Dr Jennifer Sauter is our incoming PPS Awards Committee Chair, overseeing the PPS Trainee Research, Travel, and Lifetime Achievement Awards through to 2028. Our members are encouraged to apply for Travel Awards, gaining the opportunity to join us at Lake Bled, meet our welcoming community, and engage in ongoing research.
The PPS website offers an extensive educational resource for you to explore, alongside ongoing new features such as the Case of the Month, organised through the Digital Content Committee Chair, Dr Matt Cecchini, and links to the Mayo Clinic journal club. The website also actively promotes our allied associations and their educational courses, and regularly hosts pulmonary pathology career opportunities.
Thank you for your membership!
Richard L Attanoos BSc MB BS FRCPath
Consultant Pathologist, University Hospital of Wales
Cardiff and Vale University NHS Health Board
Professor, School of Biosciences
Cardiff University, Wales, United Kingdom
2026 PPS Biennial Meeting Handouts (requires membership login)
2026 PPS Biennial Videos.
The PPS Biennial videos are now available to registrants of the meeting. If you didnot register and attend the live meeting, you may purchase accesss to the videos for a reduced price at the virtual registration page. Note that this purchase provides access to
the videos, but does not include CME.
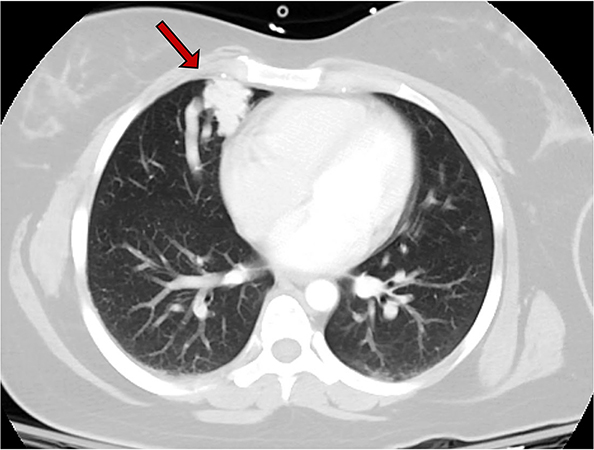
A 30-year-old woman underwent a chest computed tomography (CT) scan after a motor vehicle accident which showed an incidental 2.6 cm pulmonary ‘vascular’ lesion in the anteromedial right middle lobe (Figure 1, arrow). The patient reported symptoms of post-exertional dyspnea, intermittent mid-sternal pain, and easy bleeding. Physical exam showed clubbing of fingers but no other relevant findings. Pulmonary function tests showed a FEV1 of 2.58 (82% predicted), and DLCO of 14.17 (65% predicted). Her cardiovascular reserve was preserved with 88% SpO2 at 4 minutes in a 6-minute walk test. CT angiogram demonstrated many feeding arteries to the pulmonary lesion to allow for embolization. Subsequently, the patient underwent right middle lobectomy. Grossly, the lesion was composed of numerous vascular spaces and was relatively well-circumscribed from the adjacent lung (Figure 2). A full montage scan (Figure 3) and representative photomicrographs of the lesion at 4X magnification are shown (Figure 4, H&E; Figure 5, trichrome)..
Click here to see more.