
Click here to see all images
April, 2017
Case of the Month
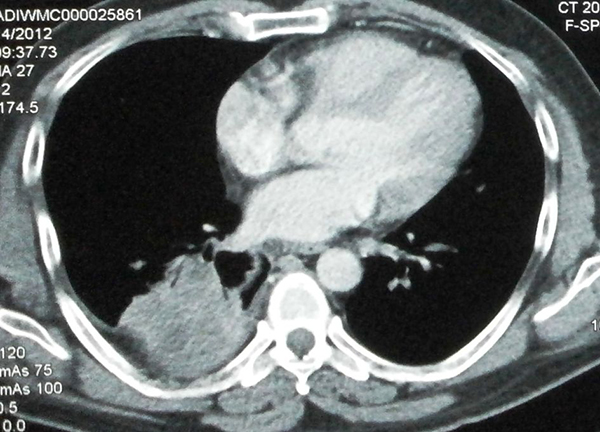
Clinical History: A 30-year-old woman presented with cough for two months and a single episode of minimal streaky hemoptysis. There was no history of recent weight loss or loss of appetite. A few days prior to presentation, she had minimal mucopurulent expectoration associated with dull aching right-sided chest pain. Physical examination revealed mildly reduced breath sounds in the right infrascapular area. Chest x-ray showed a heterogenous lesion in the right lower chest. Chest computed tomography (CT) scan showed a heterogeneous lung mass in the right lower lobe, which was regarded as suspicious for malignancy (Figure 1). Bronchoscopy showed a white membrane-like structure resembling a ruptured cyst within the airway (Figure 2). A biopsy of the membrane-like structure was performed (Figure 3).
Quiz:
Q1. Hydatid disease in humans can manifest clinically as cystic echinococcosis or alveolar echinococcosis. The latter is caused by:
- Echinococcus granulosus
- Echinococcus multilocularis
- Echinococcus vogeli
- Echinococcus equinus
- Echinococcus oligarthrus
Q2. The most common complication of hydatid cyst is:
- Infection of the cyst
- Malignant transformation
- Cyst rupture
- Fistula formation
- Calcification and calculi
Q3. The laminated membrane of a “hydatid cyst” is:
- Part of the larva
- The wall of the adult worm
- The innermost layer of a fully developed cyst
- The outermost layer of a fully developed cyst
- The layer that gives rise to brood capsules
Q4. Serology for hydatid disease of the lung is characterized by:
- Very low rate of false negative tests
- Better specificity of enzyme-linked immunosorbent assay (ELISA) than the arc 5 test
- Nearly 100% sensitivity, especially when an ELISA test is used
- Complete absence of false positive tests
- Many false-positive and false-negative results
Answers to Quiz
Q2. C
Q3. A
Q4. E
Diagnosis
Discussion
Echinococcosis can involve any organ, but the liver and lungs are most commonly affected. The right lung is affected in 60% of cases, and 60% are in the lower lobes. The larvae of E. granulosus form cysts (“hydatid cysts”) in involved parenchymal organs. On pathologic examination, the wall of an intact hydatid cyst is composed of three layers. The outermost layer (pericyst, not seen in this case) is formed by the host reaction to the parasite. The next layer, also known as the ectocyst, is most commonly encountered in practice. It is characterized by a pathognomonic laminated membrane that has a pearly-white gross appearance and a lamellated microscopic appearance (Figure 3). The innermost layer, known as the endocyst or germinative layer, was not present in this case. It is composed of several tiny scolices/protoscolices, which contain rows of distinctive hooklets (Figure 4).
Clinically, patients with a hydatid cyst of the lung often remain asymptomatic until the cyst becomes very large, causing symptoms due to compression of adjoining structures or rupture. Cyst rupture is the most common complication. In most cases, the diagnosis of echinococcosis is established by imaging and serology. However in cases of cyst rupture, imaging may be misleading, as in the present case. The sensitivity of serology for pulmonary hydatid cysts is low (60%) and there are also many false positives. The specificity increases when the arc 5 test is used instead of ELISA or indirect hemagglutination. In cases with atypical imaging or negative serology, pathologic examination is required for a definitive diagnosis.
Take home message for trainees: Pearly white membranes with a characteristic laminated appearance on histology are pathognomonic of echinococcosis.
References
Komurcuoglu B, Ozkaya S, Cirak AK et al. Pulmonary hydatid cyst: The characteristics of patients and diagnostic efficacy of bronchoscopy. Exp Lung Res 2012;38:277-80.
Lewall DB. Hydatid disease: biology, pathology, imaging and classification. Clin Radiol 1998;53:863-74.
Morar R, Feldman C. Pulmonary echinococcosis. Eur Respir J 2003;21:1069-77.
Taxy JB, Gibson WE, Kaufman MW. Echinococcosis: Unexpected Occurrence and the Diagnostic Contribution of Routine Histopathology. Am J Surg Pathol. 2017;41:94-100.
Contributors
Department of Pathology
All India Institute of Medical Sciences, New Delhi, India
Karan Madan, M.D., DM
Pulmonary Medicine & Sleep Disorders
All India Institute of Medical Sciences, New Delhi, India