
Click here to see all images
August, 2017
Case of the Month
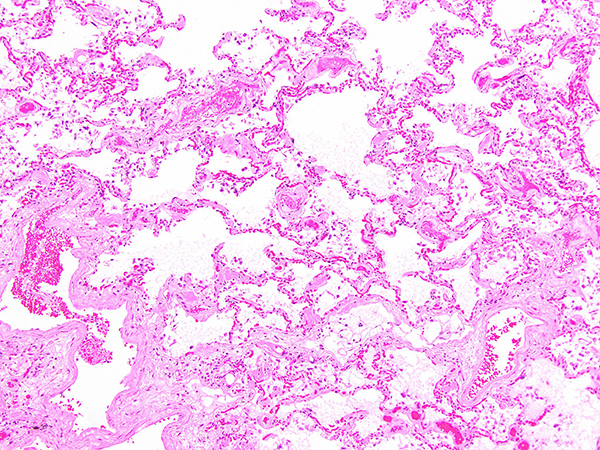
Clinical History: A 67-year-old man with a history of coronary artery disease, obstructive sleep apnea and morbid obesity sustained a right femur fracture after a fall. He underwent orthopedic surgery and had a complicated postoperative period due to respiratory insufficiency and ventilator dependance, from which he never recovered. The patient expired shortly thereafter due to respiratory failure due to diffuse alveolar damage (DAD). Representative sections of the lung from areas less involved by DAD are shown in Figures 1 through 6. A Congo red stain is shown in Figures 4 and 5 (the latter under polarized light). A representative section of the heart is shown in Figure 6.
Quiz
Q1: Which histochemical stain is most helpful for the identification of amyloid in tissue sections?
- Verhoeff-van Gieson (VVG) stain
- PAS after diastase digestion
- Congo red
- Trichrome
- Grocott
Q2: Diffuse alveolar septal amyloidosis is most frequently associated with:
- Systemic amyloidosis
- Intense inflammatory infiltrate
- Granulomatous reaction
- Interstitial fibrosis
- Honeycomb change
Q3: What is the most accurate method for subtyping amyloid?
- Immunofluorescence
- Amyloid cannot be subtype
- Polymerase chain reaction (PCR)
- Sanger sequencing
- Mass spectometry
Q4. The type of amyloid associated with senile amyloidosis is:
- Amyloid-associated protein
- Transthyretin
- Ig light chain
- Β2 microglobulin
- Calcitonin
Answers to Quiz
Q2. A
Q3. E
Q4. B
Diagnosis
Discussion
This case depicts an example of diffuse alveolar septal amyloidosis, characterized by the abnormal deposition of amyloid within alveolar septa and vessel walls. It occurs most frequently in patients with known systemic amyloidosis, but can rarely occur in patients without a prior history of extrapulmonary disease. On routine histologic sections, lung architecture is preserved with the characteristic appearance of variably thickened alveolar septa, with some areas being almost normal and others being expanded by amyloid deposits, including amyloid deposition within vessel walls. Amyloid can be differentiated from collagen deposition (interstitial fibrosis) since the former has an amorphous appearance. Involvement of blood vessels in amyloidosis is another clue to the diagnosis. Lastly, amyloid deposits are congophilic with apple-green birefringence under polarized light, which confirms the diagnosis. Immunostains to subtype the amyloid protein can be attempted, but are very difficult to interpret because of high background. Currently, mass spectometry is considered the most accurate method to subtype amyloid.
Subtyping of amyloid protein is important for treatment and prognostic purposes. Most cases of diffuse alveolar septal amyloidosis are associated with systemic AL amyloidosis. Involvement of the lung by AL amyloidosis has the worst prognosis, largely dependent on the treatment of the underlying lymphoproliferative process. Death often occurs due to involvement of the heart. ATTR amyloidosis is most frequently an incidental finding, often at the time of autopsy, of elderly individuals (>80 years of age). However, it is important to recognize it mainly because of the associated better survival and the fact that no additional treatment is required (e.g. chemotherapy).
Take home message for trainees: alveolar septal amyloidosis is generally associated with systemic amyloidosis and has a poor prognosis.
References
Govender P, Keyes CM, Hankinson EA, et al. Transbronchial biopsies safely diagnose amyloid lung disease. Amyloid 2017;24:37-41.
Khoor A, Colby TV. Amyloidosis of the Lung. Arch Pathol Lab Med 2017;141:247-54.
Contributors
Assistant Professor, Department of Pathology
University of Pittsburgh, Pittsburgh, PA