
Click here to see all images
January, 2017
Case of the Month
Clinical History:A 31-year-old man presented with chest pain and was found to have a 10-cm anterior mediastinal mass. Serum beta hCG and alpha-fetoprotein levels were normal. A needle biopsy was performed, and based on the biopsy findings, the mass was resected (Figures 1-6).
Quiz:
Q1. The differential diagnosis of an anterior mediastinal mass includes:
- Thymoma, Neurofibroma, Schwannoma, Ganglioneuroma
- Thymoma, Ganglioneuroma, Ganglioneuroblastoma, Hattori cyst
- Thymoma, Thyroid Lesion, Teratoma, Lymphoma
- Thymoma, Pericardial cyst, Bronchogenic cyst, Hattori cyst
- Thymoma, Neuroblastoma, Paraganglioma, Gastroenteric cyst
Q2. Which of the following is true regarding the tumor in this case?
- It occurs exclusively in prepubertal males
- t is almost certainly a metastasis from the testis
- A tumor with this histologic appearance cannot be a primary mediastinal neoplasm
- In this location, immature teratomas are less common than mature teratomas
- Most patients present with trichoptysis, superior vena cava syndrome or pneumothorax
Q3. On microscopic examination of these tumors:
- Skin, appendages, cartilage and fat are extremely uncommon findings
- Pancreatic tissue is a common finding
- Classification as dermoid cyst (monodermal teratoma) is common
- Bronchial and gastrointestinal mucosa are rare findings
- Granulomas are never found
Q4. Which of the following is true regarding mature mediastinal teratomas?
- They cannot be diagnosed without components derived from all three germ layers
- They never contain malignant components such as carcinoma or sarcoma
- They typically contain neural rosettes
- They most commonly occur in the middle mediastinum
- They behave in a benign fashion
Answers to Quiz
Q1. C
Q2. D
Q3. B
Q4. E
Q2. D
Q3. B
Q4. E
Diagnosis
Mature teratoma
Discussion
Teratomas are uncommon in the mediastinum, although they are often included in the radiologic differential diagnosis of anterior mediastinal masses, often recalled by the mnemonic "4Ts" (Thymic lesions, Thyroid lesions, "Terrible" lymphomas, Teratoma). Ideally, the possibility of a metastasis from a testicular or ovarian primary should be investigated clinically before assuming that a germ cell tumor is a primary mediastinal neoplasm. However, as Dr. Rosai states in his textbook: "...in the presence of a single upper mediastinal tumor with no evidence of retroperitoneal involvement the chances of this being the case are remote".
Mediastinal teratoma can occur in both sexes and at any age; however, the tumor classically presents in young adults. Many patients are asymptomatic. When symptoms are present, they are often non-specific. Presentations such as trichoptysis, superior vena cava syndrome and pneumothorax are rare. Imaging typically shows a well-circumscribed anterior mediastinal mass, often with a multilocular cystic component. The mass often protrudes into one lung field. Calcification, teeth or bone may be identifiable.
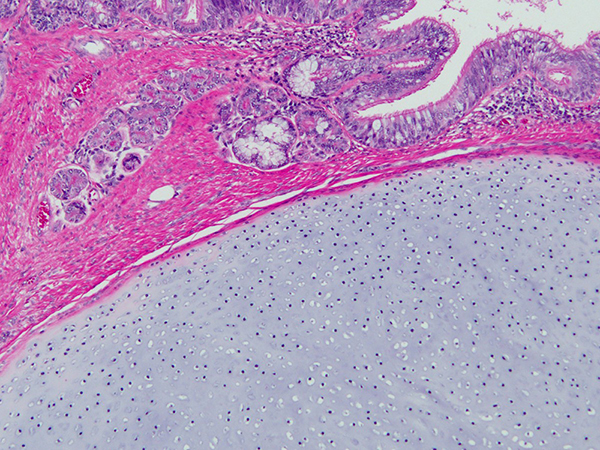
By definition, teratomas must contain tissues derived from two or three germ layers. Monodermal teratomas (dermoid cysts) are rare in the mediastinum. The most common tissues found in mediastinal teratomas are skin, cutaneous appendages, cartilage and adipose tissue (Figures 1-4). Bronchial and gastrointestinal mucosa are also common. Curiously, pancreatic tissue is a common finding in this location, unlike teratomas of other sites such as the testis (Figures 5 and 6). Granulomatous or xanthogranulomatous inflammation can occur if the cystic component ruptures.
As in other sites, teratomas can be admixed with other types of germ cell tumor, but pure teratomas do occur in the mediastinum. Mediastinal teratomas can also harbor somatic malignant components such as carcinoma or sarcoma. Immature teratomas have also been reported in this location but are far less common than mature teratomas; in a large series from Japan, only 1 of 95 cases was immature. Immature teratomas typically contain immature mesenchyme surrounding glandular epithelium or immature neuroepithelial elements (neural rosettes).
Treatment of mediastinal mature teratoma involves complete resection. Mature teratomas have an excellent prognosis regardless of age. The prognosis of pure immature teratomas is thought to be excellent in children. The prognosis of pure immature mediastinal teratomas in adults is not well established because of the low number of cases reported.
Take home message for traineees: mature teratoma can occur as a primary mediastinal neoplasm...look out for pancreatic tissue!
Mediastinal teratoma can occur in both sexes and at any age; however, the tumor classically presents in young adults. Many patients are asymptomatic. When symptoms are present, they are often non-specific. Presentations such as trichoptysis, superior vena cava syndrome and pneumothorax are rare. Imaging typically shows a well-circumscribed anterior mediastinal mass, often with a multilocular cystic component. The mass often protrudes into one lung field. Calcification, teeth or bone may be identifiable.
By definition, teratomas must contain tissues derived from two or three germ layers. Monodermal teratomas (dermoid cysts) are rare in the mediastinum. The most common tissues found in mediastinal teratomas are skin, cutaneous appendages, cartilage and adipose tissue (Figures 1-4). Bronchial and gastrointestinal mucosa are also common. Curiously, pancreatic tissue is a common finding in this location, unlike teratomas of other sites such as the testis (Figures 5 and 6). Granulomatous or xanthogranulomatous inflammation can occur if the cystic component ruptures.
As in other sites, teratomas can be admixed with other types of germ cell tumor, but pure teratomas do occur in the mediastinum. Mediastinal teratomas can also harbor somatic malignant components such as carcinoma or sarcoma. Immature teratomas have also been reported in this location but are far less common than mature teratomas; in a large series from Japan, only 1 of 95 cases was immature. Immature teratomas typically contain immature mesenchyme surrounding glandular epithelium or immature neuroepithelial elements (neural rosettes).
Treatment of mediastinal mature teratoma involves complete resection. Mature teratomas have an excellent prognosis regardless of age. The prognosis of pure immature teratomas is thought to be excellent in children. The prognosis of pure immature mediastinal teratomas in adults is not well established because of the low number of cases reported.
Take home message for traineees: mature teratoma can occur as a primary mediastinal neoplasm...look out for pancreatic tissue!
References
McKenney JK, Heerema-McKenney A, Rouse RV. Extragonadal germ cell tumors: a review with emphasis on pathologic features, clinical prognostic variables, and differential diagnostic considerations. An approach to the differential diagnosis. Adv Anat Pathol 2007;14:69-92.
Moreira AL, Chan JKC, Looijenga LHJ, et al. Mature and immature teratoma. In: Travis WD, et al. WHO classification of tumours of the lung, pleura, thymus and heart (4th edition).Lyon: IARC; 2015:257-9.
Rosai J. Germ cell tumors. In: Rosai J. Rosai and Ackerman's surgical pathology (10th edition): Mosby-Elsevier; 2011:461-3.
Shimosato Y, et al. Germ cell tumors. In: Shimosato Y, et al. AFIP atlas of tumor pathology. Tumors of the mediastinum (4th series, fascicle 11). Silver Spring, MD: ARP Press; 2010:201-8.
Takeda S, Miyoshi S, Ohta M, et al. Primary germ cell tumors in the mediastinum. A 50-year experience at a single Japanese institution. Cancer 2003;97:367-76.
Moreira AL, Chan JKC, Looijenga LHJ, et al. Mature and immature teratoma. In: Travis WD, et al. WHO classification of tumours of the lung, pleura, thymus and heart (4th edition).Lyon: IARC; 2015:257-9.
Rosai J. Germ cell tumors. In: Rosai J. Rosai and Ackerman's surgical pathology (10th edition): Mosby-Elsevier; 2011:461-3.
Shimosato Y, et al. Germ cell tumors. In: Shimosato Y, et al. AFIP atlas of tumor pathology. Tumors of the mediastinum (4th series, fascicle 11). Silver Spring, MD: ARP Press; 2010:201-8.
Takeda S, Miyoshi S, Ohta M, et al. Primary germ cell tumors in the mediastinum. A 50-year experience at a single Japanese institution. Cancer 2003;97:367-76.
Contributors
Sanjay Mukhopadhyay, M.D.
Staff Pathologist
Department of Pathology
Cleveland Clinic, Cleveland, OH, USA
Staff Pathologist
Department of Pathology
Cleveland Clinic, Cleveland, OH, USA