
Click here to see all images
April, 2018
Case of the Month
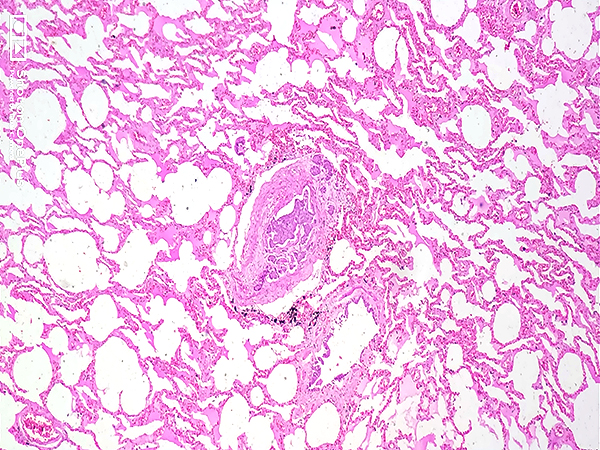
Clinical History:A 55-year-old post-menopausal woman was admitted in respiratory distress and expired within three hours. She had a three-year history of treated hypertension. She endorsed increasing shortness of breath, giddiness and easy fatigability for the preceding month. A previous echocardiograph had been normal and computed tomography (CT) revealed a bulky cervix with hydrometra, left mild hydronephrosis, retroperitoneal / bilateral iliac lymphadenopathy, sclerotic lesions in the lower lumbar vertebrae, and passive venous congestion of the liver. She was treated only symptomatically with bronchodilators. A complete autopsy was performed. Sections from the lung (Figures 1-4) and liver (Fig 5) are shown. Figure 6 is a gross photograph of the uterus and cervix.
Quiz:
Q1. Which histologic compartment of the lung does the pathologic process involve?
- Alveoli
- Bronchioles
- Blood vessels
- Pleura
- Airspaces
Q2. The histopathologic features shown here would result in failure of?
- The left ventricle
- The right ventricle
- Both ventricles
- None of the above
- Left atrium
Q3. The failure of the ventricular chamber would be
- Acute
- Subacute
- Chronic
- None of the above
- All of the above
Answers to Quiz
Q2. B
Q3. B
Diagnosis
Discussion
The proposed mechanism of PTTM is that tumor cells first metastasize to the pulmonary vessels, attach to the endothelium damaging it and activating the local coagulation system, which leads to the release of inflammatory mediators and growth factors such as tissue factor, vascular endothelial growth factor (VEGF), and platelet-derived growth factor (PDGF). In response to these growth factors, fibrocellular intimal proliferation is induced in the small pulmonary arteries and arterioles, resulting in an increase in vascular resistance.
The characteristic histopathological findings of PTTM are widespread, microscopic non-occlusive tumor emboli in the pulmonary arterioles, fibrocellular and/or fibromuscular intimal proliferation, and secondary thrombosis due to localized activation of coagulation pathways leading to luminal stenosis. The sequelae include sub-acute respiratory failure, pulmonary hypertension, right-sided heart failure, and sudden death. The fatality rate is high and it is a challenging ante-mortem diagnosis.
For unknown reasons, the most frequent histological primary tumor type is adenocarcinoma (particularly the signet ring cell type) of the stomach. PTTM associated with squamous cell carcinoma is exceedingly rare, with only five cases reported in the literature, two originating in the esophagus, two in the lung, and one in the cervix.
In the present case, sections from the lung showed tumor emboli, fibrin deposition, organized thrombi with recanalization, and fibrocellular intimal proliferation in the small pulmonary arteries. Sections from the liver showed tumor emboli in the portal vein radicle and the hepatic sinusoids. The malignant cells were squamoid with abundant eosinophilic cytoplasm and large vesicular nuclei. An endophytic tumor was identified in the cervix. The adjacent wall appeared thickened and trabeculated. Microscopically it was identified as a squamous cell carcinoma and numerous lymphovascular emboli were noted. The other organs were unremarkable. Based on these findings, the tumor emboli in the lung and liver were thought to originate from the primary tumor in the cervix.
While prognosis can be improved by an early diagnosis coupled with administration of chemotherapy, the diagnosis is often made in the post-mortem period due to the nonspecific presentation, rapid progression, and requirement of invasive procedures for a definitive diagnosis. Laboratory findings consistent with a consumptive coagulopathy, including thrombocytopenia, elevated levels of lactate dehydrogenase, and an increased INR, have been described in cases of PTTM. The CT scan findings of PTTM include multiple consolidations, ground-glass opacities, small nodular opacities, and tree-in-bud appearance in peribronchiolar areas. Ventilation-perfusion scans typically show numerous symmetric peripheral defects (“segmental contour pattern”) in contrast to pulmonary thromboembolism, which usually shows one or more, larger, and more centrally located, segmental perfusion defects. Pulmonary wedge aspiration cytology, video-assisted thoracic surgery, transbronchial lung biopsy, and CT-guided lung biopsy can help to establish the diagnosis. The definitive treatment of PTTM is chemotherapy of the underlying malignancy. The role of targeted molecular therapy by imatinib, a PDGF receptor antagonist, and bevacizumab, a VEGF receptor inhibitor, is not well established.
Take home message for trainees: PTTM should be considered in the differential diagnosis of pulmonary hypertension and subacute cor pulmonale, particularly in patients with known malignancy.
References
Okubo Y, Wakayama M, Kitahara K, et al. Pulmonary tumor thrombotic microangiopathy induced by gastric carcinoma: Morphometric and immunohistochemical analysis of six autopsy cases. Diagnostic Pathology 2011;6:27.
Roberts WC, Shafi AE, Grayburn PA, et al. Clinical and morphologic features of acute, subacute, and chronic cor pulmonale (pulmonary heart disease). Am J Cardiol 2015:115:697-703.
Tsujimoto N, Miyoshi A, Mimura M, et al. Case Report: Pulmonary Tumor Thrombotic Microangiopathy in a Cervical Cancer Patient. Gynecol Obstet Invest 2018;83:99-104.Contributors
Dr. Pradeep Vaideeswar
Dr. Kanchan Kothari
Seth GS Medical College and KEM Hospital, Mumbai, India