
Click here to see all images
July, 2018
Case of the Month
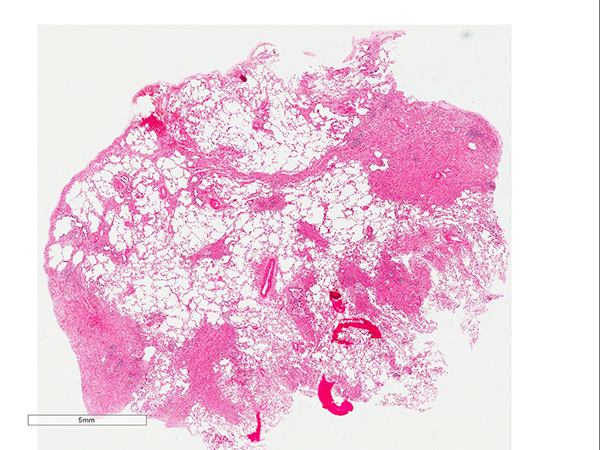
Clinical History: A 68-year-old woman with a previous history of recurrent bilateral pneumothoraces presented with shortness of breath. She had no previous smoke exposure. Serology for aspergillus precipitins and antibodies to exclude systemic diseases were negative. Chest high resolution computed tomography showed wedge-shaped bilateral dense reticular subpleural fibrosis with an upper lobe predominance and clear demarcation between the fibrosis and the normal lung. Figures 1-4 are of a surgical lung biopsy. Figures 2 and 4 are stained with an elastic von Giesson stain.
Quiz:
Q1. The predominant feature seen is:
- Pleural fibrosis
- Eosinophils
- Subleural and interalveolar fibrosis and elastosis
- Lymphoid aggregates
- Granulomas
Q2. What would be the most likely radiologic manifestations associated with these histological findings?
- Patchy consolidations
- Air entrapment
- Bilateral ground glass opacities
- Bilateral upper lobe fibrosis
- Reticulonodular densities along lymphatics
Q3. Which of the following would be associated with the findings seen in this case?
- Asthma
- Follicular bronchiolitis
- Pulmonary infiltrates
- Extravascular eosinophils
- None of the above
Q4. Which of the following pathologies would be included in the differential diagnosis?
- Apical cap
- Chronic hypersensitivity pneumonitis
- Diffuse alveolar damage
- Infection
- Acute lung injury
Answers to Quiz
Q2. D
Q3. E
Q4. A
Diagnosis
Discussion
Fig 2. Intralveolar fibrosis and elastosis highlighted with Elastic von Giesson stain.
Fig 3. Fibroblastic foci at the edge between the fibrosis and the normal lung.
Fig 4. Venous fibro-intimal thickening and fibroblastic foci.
First described in Japan by Amitani et al., pleuroparenchymal fibroelastosis (PPFE) is a rare condition that is typically an idiopathic disorder and is now recognised as such in the revised ATS/ERS classification of idiopathic interstitial pneumonias. However, PPFE has been described in association with autoimmune disorders, following recurrent infections, and in rare cases a familial component has been suggested. PPFE is also seen in the lungs of post-transplant patients, and has been reported following bone marrow and lung allografts, where it has been recently described as one form of chronic allograft dysfunction and designated restrictive allograft syndrome, as well as in patients with lung injury secondary to radiotherapy and chemotherapy. Given the number of associated conditions, it has been suggested to be a form of chronic lung injury. On radiology, the main features consist of bilateral irregular pleuroparenchymal thickening, which is typically most marked in the upper and middle zones but can spread to involve all lobes, with an associated subpleural reticular pattern and traction bronchiectasis. Very little or no honeycomb lung is noted.
The histopathological features are intra-alveolar fibroelastosis, fibroblastic foci at the leading edge of fibrosis may be present and no or mild chronic inflammation within areas of fibrosis. Granulomas should rare or not present. The key feature is the fibrosis consisting predominantly of elastic fibers and not collagen. An elastic or Movat (pentachrome) stain can help with distinguishing the predominant type of fibrosis. Vascular fibrointimal thickening of vessels is a frequent finding and pleural fibrosis can be seen occasionally. Figure one shows patchy areas of subpleural, para-septal, and bronchiolocentric fibrosis that is predominantly elastic as highlighted by an elastic von Giesson stain in figure two. The intervening alovelar parenchyma appears normal. Figure three shows intraalveolar fibrosis with fibroblastic foci at the edge between the fibrosis and normal lung. Figure four is an elastic stain highlighting venous fibrointimal thickening as well as scattered fibroblastic foci. The fibrosis is again predominantly elastic with interspersed collagen fibrosis.
The differential diagnosis includes apical cap, which shows similar histological features, but limited to the apical segments of the upper lobes. Imaging findings are key to differentiating between the two. Usual interstitial pneumonia and restrictive allograft syndrome, the latter in patients with chronic rejection after lung transplant are also in the differential along with chronic hypersensitivity pneumonitis. Usual interstitial pneumonia should always have fibroblastic foci present at the edge of the fibrosis and the composition of the fibrosis is predominantly collagen. Chronic hypersensitivity can be similar on imaging; however, the composition of the fibrosis should be predominantly collagen. Additionally, many cases will show loose non-necrotizing granulomas (although these may not always be present).
Take home message for trainees: PPFE is a rare diagnosis that can be idiopathic, occur in association with autoimmune disorders, following recurrent infections, seen after bone marrow transplantation, and in rare cases are familial. It is characterised histologically by subpleural and intra-alveolar fibrosis and elastosis of the alveolar walls, along with variable fibrous thickening of the pleura and vascular fibro-intimal thickening. A movat or elastic stain can help distinguish the elastic nature of the fibrosis.
References
Travis WD, Costabel U, Hansell DM et al. An Official American Thoracic Society/European Respiratory Society Statement: Update of the International Multidisciplinary Classification of the Idiopathic Interstitial Pneumonias. Am J Respir Crit Care Med 2013;188(6):733–48.
Reddy TL, Tominaga M, Hansell DM et al. Pleuroparenchymal fibroelastosis: A spectrum of histopathological and imaging phenotypes. Eur Respir J 2012;40(2):377–85.
Khiroya R, Macaluso C, Montero MA et al. Pleuroparenchymal Fibroelastosis: A Review of Histopathologic Features and the Relationship Between Histologic Parameters and Survival. Am J Surg Pathol 2017 Dec;41(12):1683-1689
Contributors
Histopathology Department.
Manchester University NHS Foundation Trust.
Wythenshawe Hospital. Manchester. UK.
Cristian Ortiz-Villalon M.D., Ph.D.
Pathology Department.
Karolinska University Hospitals
Stockholm. Sweden.