
Click here to see all images
August, 2019
Case of the Month
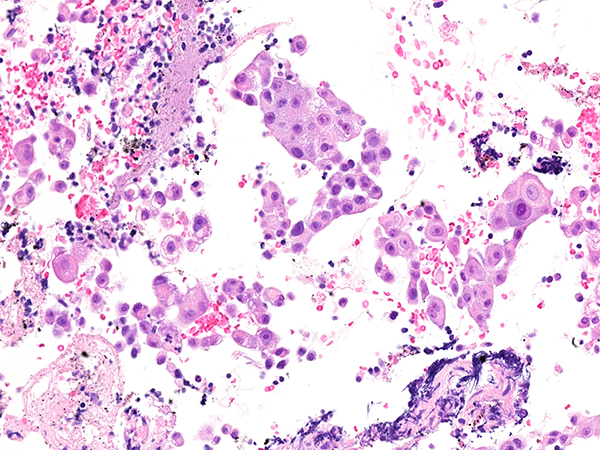
Clinical History: A 68-year-old man was found to have an incidental right lower lobe lung mass and hilar lymphadenopathy. A transbronchial biopsy was non-diagnostic and the patient subsequently had an EBUS scheduled for his 11R lymph node (Figure 1: H&E, Figure 2: TTF-1, Figure 3: napsin A, Figure 4: p40, Figure 5: alpha fetoprotein, Figure 6: HepPar1).
Quiz:
Q1. What immunohistochemical staining profile is most typical of this tumor?
- HepPar1 -, TTF-1 cytoplasmic, pCEA + (canalicular), MOC31 -, CK7 -
- HepPar1 +, TTF-1 cytoplasmic, pCEA + (non-canalicular), MOC31 +, CK7 +
- HepPar1 +, TTF-1 cytoplasmic, pCEA + (non-canalicular), MOC31 -, CK7 -
- HepPar1 +, TTF-1 cytoplasmic, pCEA + (canalicular), MOC31 +, CK7 -
Q2. What is the TTF-1 staining pattern in this tumor?
- Nuclear
- Negative
- Cytoplasmic, granular
- Perinuclear, dot-like
Q3. What is the main differential for this tumor?
- Squamous cell carcinoma
- Poorly differentiated lung adenocarcinoma
- Neuroendocrine carcinoma
- Metastatic hepatocellular carcinoma
Answers to Quiz
Q1. B
Q2. C
Q3. D
Q2. C
Q3. D
Diagnosis
Hepatoid adenocarcinoma of the lung
Discussion
Hepatoid adenocarcinoma (HAC) of the lung is a rare aggressive primary lung neoplasm with aberrant hepatocellular differentiation, often with alpha-fetoprotein production. HAC can be seen as a primary tumor in other extrahepatic organs with the most common sites including gastric (63%), ovaries (10%), and lung (5%). Less common sites include gallbladder, pancreas, uterus, and testis. This tumor is seen in heavy smokers with a median age of 64 and has a preponderance of males (2.4 to 1) with a poor outcome. The medial overall survival is 11 months.
Histologically, HAC most often mimics hepatocellular carcinoma. The cells have eosinophilic cytoplasm, round nuclei, and have a meshwork of vascular spaces. The original description of this entity described it as a lung tumor with a component of hepatocellular adenocarcinoma type architecture seen in an otherwise typical acinar and/or papillary adenocarcinoma of the lung. Signet ring differentiation and neuroendocrine morphologies have also been described. These lesions were also originally found to secrete alpha fetoprotein (AFP); however, this is not a criterion for diagnosis and many cases do not secrete or stain for AFP. In patients that do have AFP production, the levels are often extremely high and can be utilized as a method to track recurrence and if a complete resection was achieved. For cases that are negative for AFP diagnosis can be made with the aid of hepatoid morphology together with positive HepPar 1 immunohistochemistry.
The hepatoid morphology can often be missed or not apparent, especially on small biopsies, and the first clue to this diagnosis is often a granular cytoplasmic staining with TTF-1. This should prompt staining for HepPar1 and AFP. The most important differential is a metastatic hepatocellular carcinoma. MOC31 and CK7 should be positive in HAC and negative in HCC. Polyclonal CEA will be positive in a non-canalicular pattern in HAC and positive in a canalicular pattern in metastatic HCC. This is an important differentiation to make as 15% of HCC cases metastasize and 47% of those mets are to the lung.
Classification of this rare tumor, often missed or called a poorly differentiated lung adenocarcinoma without TTF-1 expression, is important as these lesions have a poorer prognosis than many lung adenocarcinomas. They often present with lymphadenopathy and/or distant metastases. Additionally, there is a potential for targeted therapy that may otherwise be missed. Hepatoid architecture is an independent predictor for ROS1-rearranged advanced non-small cell lung cancers. They have also show ALK gene rearrangements. Therefore, these patients may benefit from crizotinib (tyrosine kinase inhibitor) therapy.
Take home messages for trainees: Hepatoid adenocarcinoma of the lung is a rare aggressive primary neoplasm of the lung that is histologically similar to metastatic hepatocellular carcinoma. The first clues are hepatoid morphology and/or granular cytoplasmic TTF-1 staining.
Histologically, HAC most often mimics hepatocellular carcinoma. The cells have eosinophilic cytoplasm, round nuclei, and have a meshwork of vascular spaces. The original description of this entity described it as a lung tumor with a component of hepatocellular adenocarcinoma type architecture seen in an otherwise typical acinar and/or papillary adenocarcinoma of the lung. Signet ring differentiation and neuroendocrine morphologies have also been described. These lesions were also originally found to secrete alpha fetoprotein (AFP); however, this is not a criterion for diagnosis and many cases do not secrete or stain for AFP. In patients that do have AFP production, the levels are often extremely high and can be utilized as a method to track recurrence and if a complete resection was achieved. For cases that are negative for AFP diagnosis can be made with the aid of hepatoid morphology together with positive HepPar 1 immunohistochemistry.
The hepatoid morphology can often be missed or not apparent, especially on small biopsies, and the first clue to this diagnosis is often a granular cytoplasmic staining with TTF-1. This should prompt staining for HepPar1 and AFP. The most important differential is a metastatic hepatocellular carcinoma. MOC31 and CK7 should be positive in HAC and negative in HCC. Polyclonal CEA will be positive in a non-canalicular pattern in HAC and positive in a canalicular pattern in metastatic HCC. This is an important differentiation to make as 15% of HCC cases metastasize and 47% of those mets are to the lung.
Classification of this rare tumor, often missed or called a poorly differentiated lung adenocarcinoma without TTF-1 expression, is important as these lesions have a poorer prognosis than many lung adenocarcinomas. They often present with lymphadenopathy and/or distant metastases. Additionally, there is a potential for targeted therapy that may otherwise be missed. Hepatoid architecture is an independent predictor for ROS1-rearranged advanced non-small cell lung cancers. They have also show ALK gene rearrangements. Therefore, these patients may benefit from crizotinib (tyrosine kinase inhibitor) therapy.
Take home messages for trainees: Hepatoid adenocarcinoma of the lung is a rare aggressive primary neoplasm of the lung that is histologically similar to metastatic hepatocellular carcinoma. The first clues are hepatoid morphology and/or granular cytoplasmic TTF-1 staining.
References
Grossman K, Beasley MB, Braman SS. Hepatoid adenocarcinoma of the lung: Review of a rare form of lung cancer. Respir Med 2016;119:175-9.
Motooka Y, Yoshimoto K, Semba T, et al. Pulmonary hepatoid adenocarcinoma: report of a case. Surg Case Rep 2016;2(1):1.
Sun JN, Zhang BL, Li LK, et al. Hepatoid adenocarcinoma of the lung without production of α-fetoprotein: A case report and review of the literature. Oncol Lett 2016;12(1):189-194.
Zhao J, Zheng J, Kong M, et al. Advanced lung adenocarcinomas with ROS1-rearrangement frequently show hepatoid cell. Oncotarget 2016;7(45):74162-70.
Motooka Y, Yoshimoto K, Semba T, et al. Pulmonary hepatoid adenocarcinoma: report of a case. Surg Case Rep 2016;2(1):1.
Sun JN, Zhang BL, Li LK, et al. Hepatoid adenocarcinoma of the lung without production of α-fetoprotein: A case report and review of the literature. Oncol Lett 2016;12(1):189-194.
Zhao J, Zheng J, Kong M, et al. Advanced lung adenocarcinomas with ROS1-rearrangement frequently show hepatoid cell. Oncotarget 2016;7(45):74162-70.
Contributor
Yasmeen M. Butt, MD
Assistant Professor
Department of Pathology
University of Texas Southwestern, Dallas, TX
USA
Assistant Professor
Department of Pathology
University of Texas Southwestern, Dallas, TX
USA