
Click here to see all images
December, 2019
Case of the Month
Clinical History: A 74-year-old man, status post bilateral lung transplant in 2012 was found to have multiple bilateral pulmonary nodules on surveillance imaging. A PET CT scan demonstrated some increased metabolic uptake in a right upper lobe nodule which was subsequently biopsied. Representative images of H&E stained sections and ancillary studies performed are shown (Figures 1-6; Figure 4: smooth muscle actin; Figure 5: In-situ hybridization (ISH) for Epstein-Barr virus-encoded RNA (EBER).
Diagnosis
Quiz:
Q1. This tumor can be seen in which of the following clinical settings?
- Human immunodeficiency virus infection
- Congenital immunodeficiency
- Post transplant
- All of the above
Q2. Which of the following tests would help confirm the suspicion of this tumor in the right clinical setting?logic and immunohistochemical features of this entity include:
- HHV-8 immunostaining
- EBV-encoded RNA in situ hybridization
- MET amplification
- Acid fast stain
Q3. State true or false.
In this condition, the presence of concurrent lesions in the same or other organs is not considered definitive evidence of metastasis
Answers to Quiz
Q2. B
Q3. True
Discussion
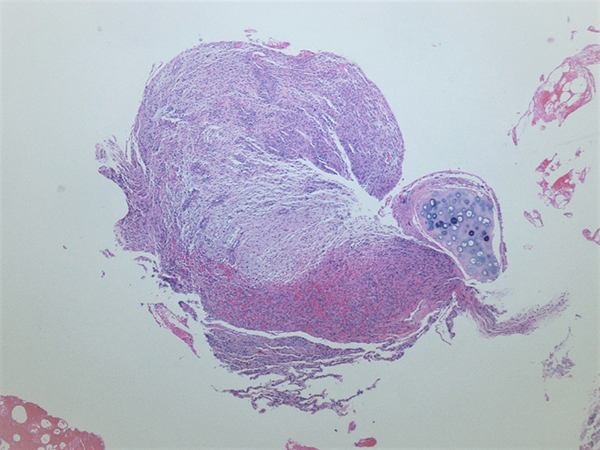
Histologically, the tumor cells show a dual population composed of fusiform to spindle shaped cells with areas of so called primitive round cells (Figures 1-3) arising gradually or abruptly from them. Immunophenotypically, a smooth muscle immunophenotype is exhibited showing variable positivity with alpha-smooth muscle actin (Figure 4), muscle specific actin and desmin. A variable lymphocytic infiltrate composed primarily of T-cells is usually seen. Variable areas of cellular atypia, mitosis and necrosis can be seen. However, the behavior of the EBV-SMT’s does not correlate well with histologic features. Demonstration of EBV-encoded RNA by in situ hybridization shows nuclear positivity in the lesional cells (Figure 5) and is critical for the diagnosis.
Typically, these tumors are relatively well differentiated, exhibiting a modest degree of nuclear atypia in contrast to most leiomyosarcomas, which frequently exhibit marked pleomorphic areas. The differential diagnosis in a spindle cell predominant lesion is Kaposi sarcoma and mycobacterial spindle cell psuedotumor. Kaposi sarcoma shows immunoreactivity with CD34 and HHV-8 and is negative for smooth muscle markers whereas the latter will show numerous acid-fast bacilli within the spindle cells. Another differential to consider is myopericytoma, as the EBV-associated SMT may contain myopericytoma-like areas characterized by multilayered concentric growth around blood vessels (Figure 6). Myopericytoma is also positive for alpha-SMA and desmin but EBV-encoded RNA in-situ hybridization will help in differentiating this neoplasm from EBV-SMTs.
Multiple tumors in a given patient have been found to be clonally distinct, supporting the view that multifocal tumors arise from multiple infectious events rather than metastases. Post-transplant patients with EBV-SMT can exhibit improvement after reduction in immunotherapy. Most solitary tumors are best managed by surgical excision. Chemotherapy and radiotherapy may be useful in cases where the tumor is unresectable.
Take home message for trainees: There should be a high index of suspicion for EBV-SMT in immunosuppressed individuals. ISH for EBER helps clinch the diagnosis.
References
Deyrup AT, Lee VK, Hill CE, et al. Epstein-Barr virus-associated smooth muscle tumors are distinctive mesenchymal tumors reflecting multiple infection events: a clinicopathologic and molecular analysis of 29 tumors from 19 patients. Am J Surg Pathol 2006; 30:75-82.
Contributor
Assistant Professor
Department of Pathology
Temple University Hospital
Philadelphia, PA.
Nikolina Dioufa, MD
PGY-3
Department of Pathology
Temple University Hospital
Philadelphia, PA.