
Click here to see all images
May, 2019
Case of the Month
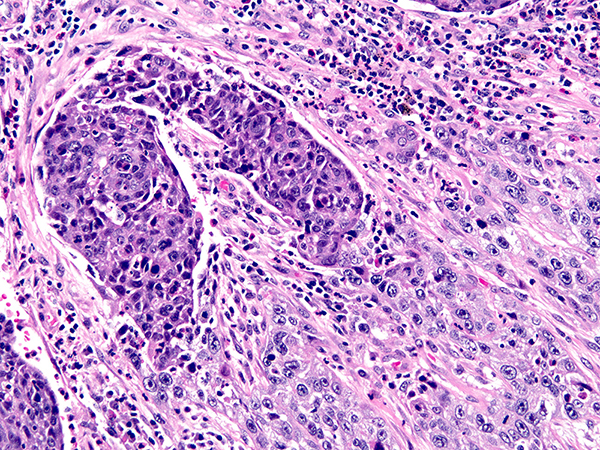
Clinical History: A 60-year-old man with a lung mass underwent EBUS-TBNA followed by lobectomy and mediastinal lymph node dissection for lung cancer. Sections from the lung mass are shown in Figures 1 and 2. A section of the background lung is shown in
Figure 3. Mediastinal lymph nodes are in Figures 4-6.
Quiz:
Q1. Which of the following statements is true regarding p40 and p63 in the subtyping of poorly differentiated non-small lung carcinoma?
- p40 is more sensitive for squamous cell carcinoma than p63
- p40 is more specific for squamous cell carcinoma than p63
- Focal positivity for p40 excludes lung adenocarcinoma
- In squamous cell carcinomas, p40 positivity confirms a lung primary
Q2. Which of the following is true regarding LEF-1?
- Among B-cell lymphomas, LEF-1 positivity is seen exclusively in CLL
- LEF-1 positivity is seen exclusively in hematologic malignancies
- LEF-1 is normally expressed in mature T cells
- LEF-1 staining has been reported in 15-30% of cases of CLL
Q3. Fragments of benign cartilage within mediastinal lymph nodes are:
- Common in mediastinal lymph nodes that have not undergone prior aspiration or biopsy
- Highly suspicious for metastatic low-grade chondrosarcoma unless proven otherwise
- The result of contamination of lymph node tissue by floaters picked up from water baths
- A biopsy site change caused by EBUS-TBNA
Answers to Quiz
Q1. B
Q2. C
Q3. D
Q2. C
Q3. D
Diagnosis
Lung: poorly differentiated squamous cell carcinoma and chronic lymphocytic B-cell leukemia/small lymphocytic lymphoma
(CLL)
Mediastinal lymph nodes: CLL and EBUS-TBNA-related biopsy site change
Mediastinal lymph nodes: CLL and EBUS-TBNA-related biopsy site change
Discussion
Both p63 and p40 can be used as squamous markers in the subtyping of non-small cell lung carcinomas that cannot be subtyped on H&E, especially when staining is strong and diffuse. Both markers have equivalent sensitivity for squamous cell carcinoma, being positive in essentially all poorly differentiated squamous cell carcinomas of the lung. In terms of specificity, p40 is superior to p63, in that it stains a lower proportion of adenocarcinomas (3% vs. 31%). Even with this increased specificity, rare cases of lung adenocarcinoma can stain focally with p40. Neither p63 nor p40 have a role in determining site of origin of squamous cell carcinoma.
This case illustrates that Occam’s razor is not always true, especially in lung pathology. Multiple unrelated disease processes can be encountered in the same lung, especially in surgical resections, and pathologists should be open to this possibility. In the current case, in addition to squamous cell carcinoma, CLL was diagnosed on the basis of the findings in the mediastinal nodes and background lung. Lymphoid enhancer-binding factor 1 (LEF-1) is a relatively new nuclear marker used in the diagnosis of CLL. It is normally expressed in mature T cells and pro-B cells, and downregulated in mature B cells. It is positive in a majority of cases of CLL (70-96%) but infrequent in other low-grade B-cell lymphomas that enter the differential diagnosis, making it a useful marker in this setting.
Figure 6 of this case illustrates a biopsy site change that has only been recently recognized. Dr. Lara Pijuan, a pulmonary pathologist and cytopathologist from Spain, was the first to report this phenomenon in 2016 in a case report that related the presence of cartilage within lymph node parenchyma to prior endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA). Pathologists from other countries subsequently noted similar findings and shared them online, where this finding came to be informally termed “Lara’s lesion”. A subsequent multi-institution international collaboration resulted in validation of this finding by demonstrating that it occurs in 11.4% of cases that have previously undergone EBUS-TBNA but not in those without a prior biopsy. It is thought that this phenomenon is caused by direct implantation of cartilage from the bronchial wall via the lumen of the biopsy needle into mediastinal lymph node tissue.
Teaching Point for Trainees:
Displaced cartilage fragments within the parenchyma of mediastinal lymph nodes are a recently recognized biopsy site change following EBUS-TBNA.
This case illustrates that Occam’s razor is not always true, especially in lung pathology. Multiple unrelated disease processes can be encountered in the same lung, especially in surgical resections, and pathologists should be open to this possibility. In the current case, in addition to squamous cell carcinoma, CLL was diagnosed on the basis of the findings in the mediastinal nodes and background lung. Lymphoid enhancer-binding factor 1 (LEF-1) is a relatively new nuclear marker used in the diagnosis of CLL. It is normally expressed in mature T cells and pro-B cells, and downregulated in mature B cells. It is positive in a majority of cases of CLL (70-96%) but infrequent in other low-grade B-cell lymphomas that enter the differential diagnosis, making it a useful marker in this setting.
Figure 6 of this case illustrates a biopsy site change that has only been recently recognized. Dr. Lara Pijuan, a pulmonary pathologist and cytopathologist from Spain, was the first to report this phenomenon in 2016 in a case report that related the presence of cartilage within lymph node parenchyma to prior endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA). Pathologists from other countries subsequently noted similar findings and shared them online, where this finding came to be informally termed “Lara’s lesion”. A subsequent multi-institution international collaboration resulted in validation of this finding by demonstrating that it occurs in 11.4% of cases that have previously undergone EBUS-TBNA but not in those without a prior biopsy. It is thought that this phenomenon is caused by direct implantation of cartilage from the bronchial wall via the lumen of the biopsy needle into mediastinal lymph node tissue.
Teaching Point for Trainees:
Displaced cartilage fragments within the parenchyma of mediastinal lymph nodes are a recently recognized biopsy site change following EBUS-TBNA.
References
Bishop JA, Teruya-Feldstein J, Westra WH, et al. p40 (ΔNp63) is superior to p63 for the diagnosis of pulmonary squamous cell carcinoma. Mod Pathol 2012;25(3):405-15.
Doxtader EE, Pijuan L, Lepe M, et al. Displaced cartilage within lymph node parenchyma is a novel biopsy site change in resected mediastinal lymph nodes following EBUS-TBNA. Am J Surg Pathol 2019;43:497-503.
Martin-Ontiyuelo C, Pijuan L, Sanchez-Font A. Piece of cartilage detected in a lymph node introduced by endobronchial ultrasound-guided transbronchial needle aspiration. Archivos de Bronchoneumologia 2016;52:560.
Menter T, Trivedi P, Ahmad R, et al. Diagnostic utility of lymphoid enhancer binding factor 1 immunohistochemistry in small B-Cell lymphomas. Am J Clin Pathol 2017;147:292-300.
Mukhopadhyay S, Katzenstein AL. Subclassification of non-small cell lung carcinomas lacking morphologic differentiation on biopsy specimens: utility of an immunohistochemical panel containing TTF-1, napsin A, p63 and CK5/6. Am J Surg Pathol 2011; 35:15-25.
Doxtader EE, Pijuan L, Lepe M, et al. Displaced cartilage within lymph node parenchyma is a novel biopsy site change in resected mediastinal lymph nodes following EBUS-TBNA. Am J Surg Pathol 2019;43:497-503.
Martin-Ontiyuelo C, Pijuan L, Sanchez-Font A. Piece of cartilage detected in a lymph node introduced by endobronchial ultrasound-guided transbronchial needle aspiration. Archivos de Bronchoneumologia 2016;52:560.
Menter T, Trivedi P, Ahmad R, et al. Diagnostic utility of lymphoid enhancer binding factor 1 immunohistochemistry in small B-Cell lymphomas. Am J Clin Pathol 2017;147:292-300.
Mukhopadhyay S, Katzenstein AL. Subclassification of non-small cell lung carcinomas lacking morphologic differentiation on biopsy specimens: utility of an immunohistochemical panel containing TTF-1, napsin A, p63 and CK5/6. Am J Surg Pathol 2011; 35:15-25.
Contributor
Sanjay Mukhopadhyay, M.D.
Director of Pulmonary Pathology
Cleveland Clinic, Cleveland, OH
Director of Pulmonary Pathology
Cleveland Clinic, Cleveland, OH