
Click here to see all images
October, 2019
Case of the Month
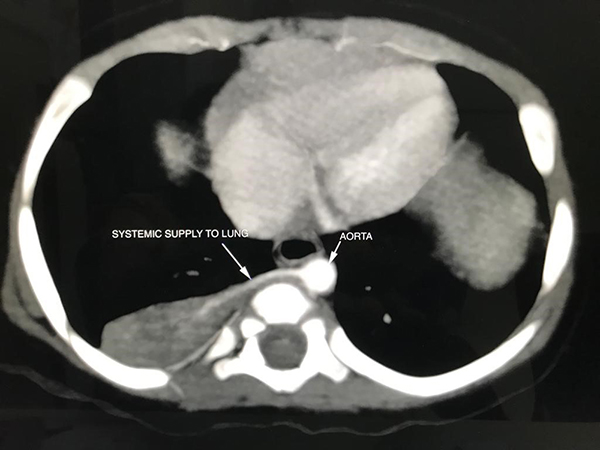
Clinical History: A 9-month-old asymptomatic girl underwent a right postero-lateral thoracotomy with excision of a right-sided (antenatally identified) non-functioning lung segment, which was demonstrated to have a systemic blood supply on preoperative imaging (Figure 1). On gross examination, the specimen measured 45 × 30 × 08 mm, was completely covered by pleura externally and showed yellowish firm areas and tiny cysts measuring 1-5 mm on cut section (Figure 2). H&E stained sections from the lung segment are shown at varying magnifications (Figures 3-6).
Quiz:
Q1. Which germ layer does the lung bud develop from?
- Ectoderm
- Mesoderm
- Endoderm
- None of the above
Q2. Which congenital lung disease shows an aberrant systemic arterial blood supply?
- Pulmonary sequestration
- Congenital pulmonary airway malformation
- Congenital lobar emphysema
- None of the above
Q3. Which subtype of pulmonary sequestration is invested by its own pleura?
- Extralobar pulmonary sequestration
- Intralobar pulmonary sequestration
- Both
- Neither
Answers to Quiz
Q2. A
Q3. A
Diagnosis
Discussion
Congenital lung diseases are a group of diverse, yet related anomalies, which can broadly involve the bronchopulmonary tree (lung bud), pulmonary vasculature, or a combination of both. Congenital diseases of the lungs are best understood in the context of normal development.
Briefly, the lung buds are endodermal in origin and develop from the primitive foregut. They are enveloped in mesenchyme throughout development. The airways are formed by dichotomous and asymmetric branching followed by branching morphogenesis of the lung buds due to chemical gradients present in the mesenchyme. Blood vessels simultaneously develop ‘de novo’ within the mesenchyme by the process of vasculogenesis eventually forming a plexus which is connected initially to the primitive branchial arteries. After the pulmonary arteries develop by angiogenesis from the aortic sac, the plexus is reconnected to the pulmonary vasculature with regression of the previously established systemic connections. Remodeling and thinning of the interface between the alveolar sacs and the pulmonary capillaries in the later stages of development, facilitates gas exchange. The entire process is regulated by complex molecular interactions between the mesenchymal and endodermal components.
PSs are localized lesions showing both bronchopulmonary and vascular anomalies. They are extremely rare, with no published population incidence. In these lesions, the non-functioning lung parenchyma receives its blood supply via an aberrant systemic artery and continuity of the lesion with the upper respiratory tract cannot be demonstrated. PSs are further classified as extra-lobar (EPS) or intra-lobar (IPS), the former being invested by its own pleura. CPAM also called congenital cystic adenomatoid malformation (CCAM) is considered to be primarily a bronchopulmonary anomaly. The incidence ranges from 1 in 11,000 to 1 in 35,000 live births. It is characterized by the presence of anomalous bronchiolar or acinar structures. Since the lesion may or may not be cystic, the former term is preferred over the latter. These lesions are generally poorly delineated from the adjacent normal lung parenchyma.
The co-occurrence of EPS and CPAM, as seen in the present case, may be the result of abnormal regulation of the interactions between the mesenchymal and endodermal components at a specific time point, likely during the pseudo-glandular phase of lung development which spans 7 to 17 weeks of gestation, leading to the altered development of both components.
Take home message
Congenital diseases of the lungs are best understood in the context of normal histology and development. A multi-disciplinary approach is essential to reach the correct diagnosis.
References
Kotecha S, Barbato A, Bush A, et al. Antenatal and postnatal management of congenital cystic adenomatoid malformation. Paediatr Respir Rev 2012;13:162-71.
Langston C. New concepts in the pathology of congenital lung malformations. Semin Paediatr Surg 2003;12:17-37.
Mastrogiulio MG, Barone A, Disanto MG, et al. Type II congenital pulmonary airway malformation associated with intralobar pulmonary sequestration: report of a case and review of classification criteria. Pathologica 2016;108:38-41.
Contributor
Dr. Alpa Bharati
Dr. Parag Karkera
Bai Jerbai Wadia Hospital for Children, Mumbai, India