
Click here to see all images
September, 2019
Case of the Month
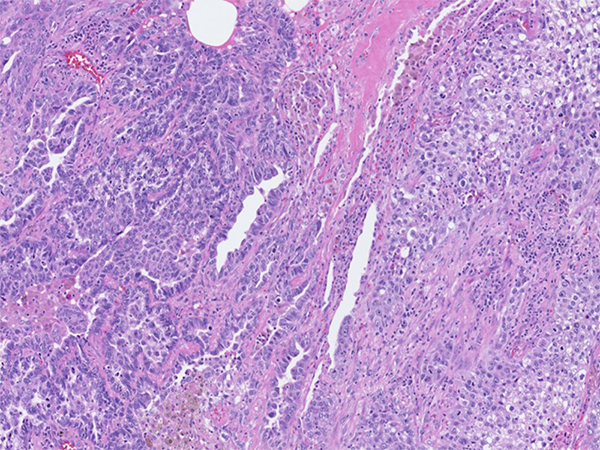
Clinical History: A 73-year-old man was seen in the emergency room for neck and cheek swelling, which turned out to be a blocked salivary duct which eventually resolved. During this visit, it was noted that he had a right upper lobe lung lesion on chest CT imaging. He was a firefighter and continued to smoke a half a pack per day for the last 25-30 years. Later, he underwent wedge resection (Figures 1-3 H&E, 4-7 TTF-1/p40) followed by completion lobectomy of the right upper lobe of lung.
Genomic DNA extracted from this tumor was analyzed to detect somatic variants on 50 genes using next generation sequencing (NGS), which showed only TP53 mutation without any EGFR, KRAS or BRAF mutations. ALK, RET and ROS1 rearrangements were also negative. Later the patient had metastatic disease to several sites including liver, pancreas and chest wall. PD-L1 testing for the clone 22C3 pharmDX showed tumor proportion score of 70%.
Quiz:
Q1. Which of the following is true to this lesion?
- Mixed histology of squamous and adenocarcinoma
- Less aggressive subtype
- Seen in non-smokers
- Harbors MAML2 rearrangement
Q2. Immunohistochemical profile of this lesion is best suited to,
- Cytokeratins (+), glands p40 (+), solid component p40 (+)
- Cytokeratins (+), glands TTF-1 (+), solid component p40 (+)
- Cytokeratins (+), glands TTF-1 (+), solid component p40 (-)
- Cytokeratins (-), glands TTF-1 (-), solid component p40 (-)
Q3. Which of the following clones of PD-L1 should be utilized in this setting if pembrolizumab (KEYTRUDA) therapy is being considered?
- SP142
- 28-8
- 22C3
- SP263
Answers to Quiz
Q2. B
Q3. C
Diagnosis
Discussion
Genetic analyses of adenosquamous carcinoma have shown mutations of EGFR and KRAS more commonly than others. ALK and ROS1 rearrangements and HER2 mutations are seen in a few cases. Molecular testing is of paramount importance to guide the need for targeted therapies.
Several PD-L1 immunohistochemistry (IHC) tests are commercially available to detect the PD-L1 protein. United States (US) Food and Drug Administration (FDA) recommends 22C3-IHC testing for treatment selection for administration of pembrolizumab therapy. The other IHC antibody clones such as 28-8, SP142 and SP263 are used for nivolumab, atezolizumab and durvalumab treatment selections respectively.
Take home message
Positivity for TTF-1 in malignant glands and p40 in the solid component supports the diagnosis of adenosquamous carcinoma.
References
2. Travis WD, et al. WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart. WHO Classification of Tumours, 4th Edition, Volume 7, 2015.
3. Udall et al. PD-L1 diagnostic tests: a systematic literature review of scoring algorithms and test-validation metrics. Diagnostic Pathology 2018;13(1):12.
Contributor
Assistant Professor of Pathology
Pulmonary Pathologist
Director, Immunohistochemistry
Department of Pathology
Virginia Commonwealth University
Richmond, VA