
Click here to see all images
March, 2020
Case of the Month
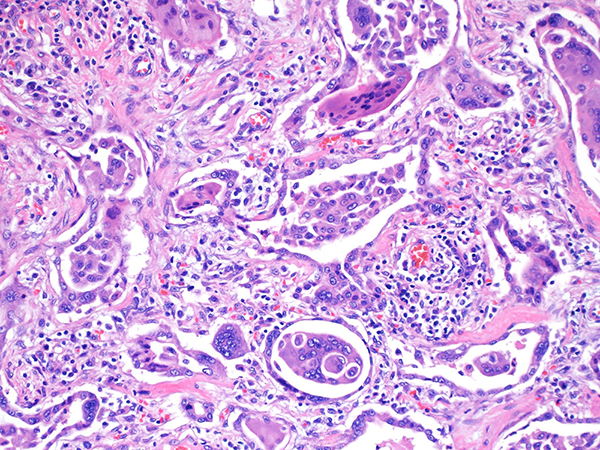
Clinical History: A 21-year-old male, never smoker, presented with severe productive cough and progressive dyspnea for a year. He works in a tool and die factory grinding metal for the past 3 years. His workup for rheumatologic and infectious diseases is negative. A high-resolution chest CT scan compared to a prior CT from 3 months earlier showed right-sided pneumothorax (iatrogenic) and rapidly progressive pulmonary fibrosis with a slight upper lobe predominance (Figure 1). Lung biopsy findings are shown in Figures 2-5.
Quiz:
Q1. The characteristic cell type seen in this entity is:
- Macrophages
- Eosinophils
- Giant cells
- Lymphocytes
- A and C
Q2. All are correct except:
- This disease is an airway-centered process
- The multinucleated giant cells typically show emperipolesis
- Numerous pigmented histocytes forming small collagenous nodules are often found
- Patients have history of working with a mixture of tungsten carbide and cobalt
- Desquamative interstitial pneumonia should be considered in the differential diagnosis.
Q3. Under polarized light, birefringent silica particles are present.
- True
- False
Answers to Quiz
Q1. E
Q2. C
Q3. False
Q2. C
Q3. False
Diagnosis
Hard Metal Pneumoconiosis
Discussion
Hard metal is composed of a mixture of tungsten carbide and cobalt. Occasionally, small amounts of other metals including titanium, tantalum, chromium, and nickel can also be found. Hard metal is used in various industries because of its stiffness and resistance to high temperatures and exposures are usually in the setting of grinding or drilling of tools as well as polishing diamond. Of note, our patient was grinding metal, specifically tungsten carbide and cobalt without any protection for a significant period of time. Hard metal lung disease is more likely to occur in poorly regulated workplaces, but its occurrence depends mainly on individual susceptibility, rather than on cumulative exposure, so even young subjects may be affected.
Clinically, patients present with cough and dyspnea and diffuse lung infiltrates on imaging. Histologically, hard metal pneumoconiosis (HMP) is characterized by marked interstitial fibrosis and cellular interstitial infiltrates that are more centered around bronchioles (Figs. 2 and 3) with a predominance of alveolar space giant cells. Therefore, HMP is also known as giant cell interstitial pneumonia (GIP). GIP is almost always associated with hard metal pneumoconiosis, however, rare cases with no history of hard metal exposure have been described. In cases with no exposure history, GIP should be the diagnosis rather than HMP. The key finding in HMP/GIP is the presence of prominent collections of intra-alveolar macrophages and large multinucleated giant cells (Fig. 4), some showing emperipolesis highlighted by the arrow (Fig. 5). Microanalytic studies can identify tungsten in the tissue, but cobalt which is considered the main etiologic agent is water soluble and usually not present after processing. Collagenous nodules with pigmented macrophages and polarizable silica are seen in mixed dust fibrosis and not HMP.
The differential diagnosis includes respiratory bronchiolitis/desquamative interstitial pneumonia, however, the presence of large multinucleated giant cells within the alveolar spaces with focal cannibalism as well as alveolar septal chronic inflammation and/or fibrosis should exclude these diagnoses. Clinical history of hard metal exposure would be helpful in arriving at the correct diagnosis.
Recovery may happen after elimination of exposure, although death can occur due to progressive disease. This patient underwent a double lung transplant shortly after diagnosis.
Take home message for trainees: The finding of giant cell interstitial pneumonia is almost pathognomonic of hard-metal disease and should provoke an investigation of occupational exposure.
Clinically, patients present with cough and dyspnea and diffuse lung infiltrates on imaging. Histologically, hard metal pneumoconiosis (HMP) is characterized by marked interstitial fibrosis and cellular interstitial infiltrates that are more centered around bronchioles (Figs. 2 and 3) with a predominance of alveolar space giant cells. Therefore, HMP is also known as giant cell interstitial pneumonia (GIP). GIP is almost always associated with hard metal pneumoconiosis, however, rare cases with no history of hard metal exposure have been described. In cases with no exposure history, GIP should be the diagnosis rather than HMP. The key finding in HMP/GIP is the presence of prominent collections of intra-alveolar macrophages and large multinucleated giant cells (Fig. 4), some showing emperipolesis highlighted by the arrow (Fig. 5). Microanalytic studies can identify tungsten in the tissue, but cobalt which is considered the main etiologic agent is water soluble and usually not present after processing. Collagenous nodules with pigmented macrophages and polarizable silica are seen in mixed dust fibrosis and not HMP.
The differential diagnosis includes respiratory bronchiolitis/desquamative interstitial pneumonia, however, the presence of large multinucleated giant cells within the alveolar spaces with focal cannibalism as well as alveolar septal chronic inflammation and/or fibrosis should exclude these diagnoses. Clinical history of hard metal exposure would be helpful in arriving at the correct diagnosis.
Recovery may happen after elimination of exposure, although death can occur due to progressive disease. This patient underwent a double lung transplant shortly after diagnosis.
Take home message for trainees: The finding of giant cell interstitial pneumonia is almost pathognomonic of hard-metal disease and should provoke an investigation of occupational exposure.
References
Khoor A, Roden AC, Colby TV, et al. Giant cell interstitial pneumonia in patients without hard metal exposure: analysis of 3 cases and review of the literature. Hum Pathol 2016;50:176–82.
Mizutani RF, Terra-Filho M, Lima E, et al. Hard metal lung disease: a case series. J Bras Pneumol 2016;42:447–52.
Naqvi AH, Hunt A, Burnett BR, et al. Pathologic spectrum and lung dust burden in giant cell interstitial pneumonia (hard metal disease/cobalt pneumonitis): review of 100 cases. Arch Environ Occup Health 2008;63:51–70.
Nemery B, Verbeken EK, Demedts M. Giant cell interstitial pneumonia (hard metal lung disease, cobalt lung). Semin Respir Crit Care Med 2001;22:435–48.
Mizutani RF, Terra-Filho M, Lima E, et al. Hard metal lung disease: a case series. J Bras Pneumol 2016;42:447–52.
Naqvi AH, Hunt A, Burnett BR, et al. Pathologic spectrum and lung dust burden in giant cell interstitial pneumonia (hard metal disease/cobalt pneumonitis): review of 100 cases. Arch Environ Occup Health 2008;63:51–70.
Nemery B, Verbeken EK, Demedts M. Giant cell interstitial pneumonia (hard metal lung disease, cobalt lung). Semin Respir Crit Care Med 2001;22:435–48.
Contributor
Mitra Mehrad, M.D.
Assistant Professor
Department of Pathology, Microbiology and Immunology
Vanderbilt University Medical Center, Nashville, TN, USA
Assistant Professor
Department of Pathology, Microbiology and Immunology
Vanderbilt University Medical Center, Nashville, TN, USA