
Click here to see all images
January, 2021
Case of the Month
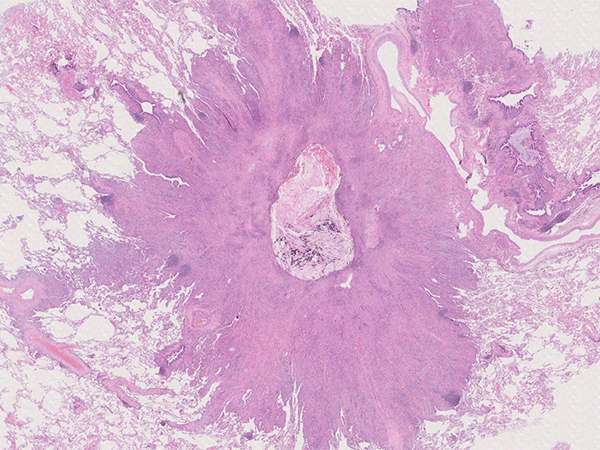
Clinical History: A 1.8-cm solitary peripheral pulmonary nodule was resected in a 72-year-old woman with long-standing rheumatoid arthritis. The clinical suspicion was carcinoma or a rheumatoid nodule. Macroscopically, the nodule was tan-white and lobulated, with central necrosis and calcification as seen in Figure 1. Histologically, the nodule consisted predominantly of cytologically bland histiocytes and multinucleated giant cells with cytoplasmic inclusions and some background fibrosis (Figure 2). The histiocytes were positive for CD163 (Figure 3). The cytoplasmic inclusions were visible as unstained rhomboid/needle-shaped cytoplasmic inclusions in the CD163 stain (Figure 3) and accentuated in the Gram stain (Figure 4).
Small lymphoid nodules consisting predominantly of CD20-positive small B cells with moderately abundant clear cytoplasm were discernible at the border of the histiocytic lesion and the lung in association with abundant plasma cells showing kappa light-chain restriction using immunohistochemical staining, and intimate association with bronchial and alveolar epithelium (Figures 5 and 6; Figure 6 includes CD3, CD20, kappa and lambda light chains).
Quiz:
Q1. What is responsible for the accumulation of histiocytes in the presented case?
- Amyloid
- Immunoglobulins
- Bacteria
- Aspirate
Q2. Which is the underlying disease?
- metabolic storage diseases
- immunosuppression
- neoplasia
- infection
Q3. Which organs are commonly affected by this rare lesion
- Lung
- Pleura
- Head and neck region
- All of the above
Answers to Quiz
Q2. C
Q3. D
Diagnosis
Discussion
CSH can occur in any organ. More than half of the cases reported have presented as localized disease, most commonly in the head and neck, lung or pleura. In contrast, generalized CSH affects the lung in only 10% of cases, and is predominantly found in the bone marrow (97%), liver (47%), lymph nodes (44%), spleen (44%), and kidneys (38%).
The lesion has no gender predilection and affects adults with a wide age range. The vast majority of cases are associated with plasma cell neoplasms or lymphomas with plasma cell differentiation. Very few cases have been described in patients with infection or autoimmune disease without hematological malignancy. Although overall rare, marginal zone lymphoma of MALT type is the most common form of primary pulmonary lymphoma. The underlying reason for the tissue phenomenon of CSH is unknown. It is speculated that mutations in the variable region promote conformational alterations of immunoglobulins and lead to crystallization.
CSH can partially or completely obscure the presence of an associated or underlying lymphoplasmacytic disorder. Although CSH without associated neoplastic disease has been described in few cases with long-standing rheumatoid arthritis, an underlying hematological malignancy is most likely to be present and needs to be thoroughly excluded.
The prognosis of CSH depends on the underlying condition and CSH is not specifically treated. Any therapy is directed against the underlying disease. In general, the prognosis of localized extranodal pulmonary marginal zone lymphoma of MALT type is excellent, and some studies suggest no difference in survival of MALT lymphoma patients compared with age- and sex-matched control patient populations.
The differential diagnosis according to the histological aspect of CSH has been nicely described by Zhang and Myers (see references), comprising:
(a) metabolic storage diseases, in particular Gaucher cells in Gaucher disease,
(b) so-called pseudo-Gaucher cells in CML,
(c) pulmonary malakoplakia, an uncommon manifestation of Rhodococcus equi infection seen almost exclusively in HIV-infected patients, (and in… have a look at the “case of the month July 2020”!)
(d) granular cell tumor of the lung,
(e) adult rhabdomyoma, and
(f) non-immunoglobulin CSH.
Non-immunoglobulin CSH comprises conditions with sheets of histiocytes with eosinophilic inclusions other than immunoglobulin light-chains, although those have not yet been described in the lung (e.g. Charcot-Leyden crystal-associated, crystals associated with clofazimine-medication or hereditary cystinosis).
Specific clinical history, morphological characteristics and immunohistochemical and histochemical staining results are used to differentiate those lesions.
Take home message: Pulmonary crystal-storing histiocytosis is a rare nodular lesion characterized by histiocytes with abundant fibrillary cytoplasmic inclusions representing immunoglobulin of light chain origin. It is most often associated with lymphoproliferative disease, which may be obscured by the histiocytic reaction.
References
Zhang C, Myers JL. Crystal-storing histiocytosis complicating primary pulmonary marginal zone lymphoma of mucosa-associated lymphoid tissue. Arch Pathol Lab Med 2013;137:1199-204.
Contributors
Associate Professor
Institute of Pathology
Lausanne University Hospital and University of Lausanne
Lausanne, Switzerland