
Click here to see all images
November, 2021
Case of the Month
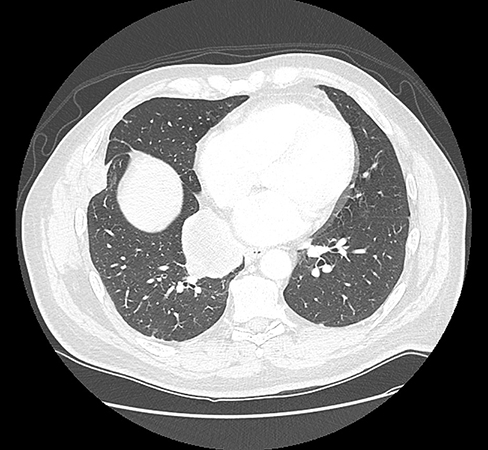
Clinical History: A 59-year-old male, never smoker, with no prior cancer history, presented with chest pain. The chest CT scan revealed a 5.5 cm solid right infrahilar lung mass (Figure 1). Representative H&E images showed undifferentiated high-grade tumor with marked necrosis, abundant mitoses, and apoptotic bodies (Figure 2). The tumor cells showed high N/C ratio, molding, and dispersed chromatin (Figures 3 and 4). Immunohistochemistry (IHC) was diffusely positive for keratin (OSCAR) (Figure 5), diffusely positive for CD56 (Figure 6), and negative for pan-cytokeratins AE1/AE3 and CAM 5.2, chromogranin, synaptophysin, INSM1, TTF-1, CD45, SOX10, S100, Melan A and HMB45. Ki67 proliferative index was more than 90%. Next-generation sequencing revealed 38 mutations including a BRAF mutation, along with abundant G>A, C>T, GG>AA, and CC>TT transition mutations, indicating a UV-exposure mutagenesis.
Q1. Even though the above morphologic features together with positive CD56 raise a consideration of small cell carcinoma, which of the following is the biggest “red flag” that should make one consider an alternative diagnosis?
- The lack of smoking history
- The lack of synaptophysin labeling
- The lack of chromogranin labeling
Q2. Which of the following statements is correct
- Lack of a known history of melanoma does not exclude the diagnosis of metastatic melanoma
- Cutaneous melanomas can present as large solitary lung metastases in the absence of a known skin primary
- UV signature can serve as a reliable marker of tumors metastatic from sun-exposed skin
- All of the above
Q3. What is the definition of undifferentiated melanoma?
- Lack of expression of routinely used melanoma immunohistochemical markers
- Lack of melanin pigment
- Variable histology from pleomorphic epithelioid to rhabdoid, spindled or primitive small round cell
- All of above
Answers to Quiz
Q2. D
Q3. D
Diagnosis
Discussion
A variety of entities should be considered in the differential diagnosis of poorly-differentiated primitive round cell tumors of the lung that resemble SCLC but arise in a never-smoker, including NUT carcinoma, SMARCA4-deficient undifferentiated tumors (usually these occur in smokers but may occasionally arise in never-smokers), various round cell sarcomas, including Ewing sarcoma, and metastatic tumors such as Merkel cell carcinoma.
Melanomas are not commonly included in the differential diagnosis of SCLC. However, undifferentiated melanomas are an extremely challenging diagnosis, and they can mimic various tumors. Dedifferentiated/undifferentiated melanomas can have a variety of morphologies, including undifferentiated pleomorphic sarcoma-like (most common), rhabdoid, spindled or primitive small round cell. Most notably, undifferentiated melanomas completely lack expression of melanocytic markers and can express cytokeratins, so when presenting as a lung mass, they can closely mimic lung carcinoma. In most cases, this issue is encountered for epithelioid melanomas mimicking non-small cell lung carcinomas, but this case illustrates a rare scenario of undifferentiated melanoma mimicking SCLC. In a recent molecular study from our group, we found that cutaneous melanomas can present as solitary large lung metastases in the absence of known primary lesions, which occurs presumably as a results of regression of primary melanoma after the metastasis has occurred.
In the current case, the diagnosis of undifferentiated melanoma could not be made based on histologic and IHC grounds alone, as is usually the case for such tumors unless the history of dedifferentiated primary melanoma is known. Given the unusual clinical setting and labeling for CD56 only, the tumor was initially classified as undifferentiated malignant neoplasm with SCLC possibility raised in a note. The diagnosis of undifferentiated melanoma was subsequently suggested by next-generation sequencing based on genomic profile highly characteristic of cutaneous melanoma, including the presence of a strong UV signature and a BRAF mutation.
This case also illustrates a pitfall of relying on CD56 (even if strong and diffuse) as a neuroendocrine marker. CD56 has been widely used in thoracic pathology for the diagnosis of SCLC; however, CD56 should be used with caution if positive in isolation since it can be strongly expressed by a variety of non-neuroendocrine neoplasms, including various hematolymphoid neoplasms, basaloid squamous cell carcinoma, various sarcomas. Notably, melanomas are commonly positive for CD56.
Take home message for trainees: Undifferentiated lung tumors resembling small cell carcinoma in never-smokers commonly represent an alternative diagnosis. The differential diagnosis is wide, but in rare instances may include an undifferentiated melanoma. One should not rely on CD56 alone as a convincing marker of neuroendocrine differentiation.
References
Agaimy A, Specht K, Stoehr R, et al. Metastatic malignant melanoma with complete loss of differentiation markers (undifferentiated/dedifferentiated melanoma): analysis of 14 patients emphasizing phenotypic plasticity and the value of molecular testing as surrogate diagnostic marker. Am J Surg Pathol 2016;40:181-91.
Gupta S, Sosa CP, Kosari F, et al. A comparison of adult rhabdomyosarcoma and high-grade neuroendocrine carcinoma of the urinary bladder reveals novel PPP1R12A fusions in rhabdomyosarcoma. Hum Pathol 2019;88:48-59.
Rekhtman N. Lung neuroendocrine neoplasms: recent progress and persistent challenges. Mod Pathol 2021; Epub ahead of print. PMID: 34663914.
Yang C, Sanchez-Vega F, Chang JC, et al. Lung-only melanoma: UV mutational signature supports origin from occult cutaneous primaries and argues against the concept of primary pulmonary melanoma. Mod Pathol 2020;33:2244-55.
Contributors
Thoracic pathology fellow
Department of Pathology
Memorial Sloan Kettering Cancer Center
Natasha Rekhtman, M.D., Ph.D.
Attending Thoracic Pathologist and Cytopathologist
Department of Pathology
Memorial Sloan Kettering Cancer Center