
Click here to see all images
July, 2022
Case of the Month
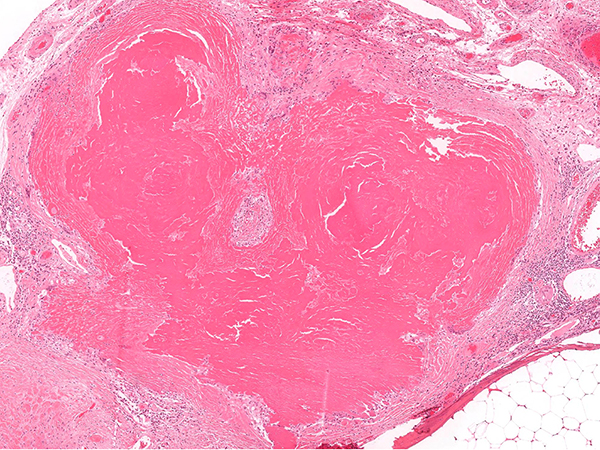
Clinical History: A 70-year-old male with adenocarcinoma in the left upper lobe. Intraoperatively an abnormality was identified on the visceral surface of the left lower lobe that was suspected intraoperatively to represent an ipsilateral metastasis of the lung cancer. An upper lobe lobectomy and wedge of the left lower lobe lesion was performed. The upper lobe demonstrated an acinar predominant adenocarcinoma. A nodular area was identified in the lower lobe and representative hematoxylin and eosin stained photomicrographs of the lesion are shown in figure 1-3. The lesion was negative for Congo Red but demonstrated strong bright crimson red staining on a Masson Trichrome (figure 4). A comparison composite is presented in figure 5 with different histochemical stains. A clonal Kappa expressing population of plasma cells was identified (figure 6). Electron microscopy demonstrated osmiophilic material forming aggregates of granular electron-dense deposits adjacent to entrapped collagen fibers (figure 7). Subsequent bone marrow and further work up did not demonstrate a systemic plasma cell neoplasm. Note: Non-relevant clinical history may have been omitted or altered to protect patient privacy.
Q1. Glassy eosinophilic deposits on hematoxylin and eosin stained sections that are negative on a Congo Red histochemical stain most likely represent which of the following?
- Light chain deposition disease (LCDD)
- Congo Red negative Amyloid
- Transthyretin Amyloid
- Non-specific fibrosis
Q2. In addition to Congo Red which of the following stains can be used to highlight amyloid?
- Periodic acid–Schiff (PAS)
- Sulfated Alcian blue
- Martius Scarlet Blue
- Movat
Q3. What is the typical appearance of amyloid on electron microscopy?
- Osmiophilic material forming aggregates of granular electron-dense deposits
- Fibrils with an average diameter of 20 nm
- Twisted protofibrils with diameters ranging 40 to 200 nm
- Non-branching fibrils with an average diameter of 7.5–10 nm
Answers to Quiz
Q2. B
Q3. D
Diagnosis
Discussion
The diagnosis of LCDD should be suspected when glassy eosinophilic deposits are identified that are negative for Congo Red staining. Since Amyloid is much more common than LCDD a practical point is to first repeat the Congo Red staining before embarking on a diagnostic (mis)adventure. It is advisable to confirm with your lab that sections stained for Congo Red have been cut as thicker sections (ideally 8-10 microns) as standard thickness sections (< 5 microns) can be falsely negative on Congo Red histochemical stains. As outlined in figure 5 some other commonly available stains (Masson and Movat) demonstrate distinct staining characteristics and can be used to help classify the eosinophilic deposits. Masson trichrome produces a visually striking strong bright crimson red staining (figure 4) in LCDD. While not available in all labs Sulfated Alcian blue can also be used to help distinguish light chain deposits with LCDD staining ‘salmon’ pink and amyloid a ‘seafoam’ green.
Since LCDD is often associated with a clonal plasma cell population. Staining for Kappa and Lambda is recommended along with hematopathology workup. In this current case there was marked Kappa restriction with aberrant co-expression of CD56 in keeping with a plasma cell neoplasm. As highlighted above nodular amyloidosis is typically associated with localized disease but additional clinical work up to better characterize the plasma cell neoplasm and systemic involvement is typically done by a consulting hematologist. Some series have also reported a pulmonary cystic disorder related to light chain deposition. Other series have described an association between Sjogren’s syndrome and LCDD that presented with multiple cystic cavities and nodules on imaging.
The diagnosis of LCDD can typically be made based on the characteristic staining patterns, however, in some case electron microscopy can be utilized to aid in distinguishing cases of amyloid. In LCDD the characteristic findings are osmiophilic material forming aggregates of granular electron-dense deposits which is distinct from the non-branching fibrils with an average diameter of 7.5–10 nm that are observed in amyloid. Mass spectrometry proteomic analysis has also been utilized by some groups to further support the diagnosis of LCDD and exclude amyloid in diagnostically challenging cases.
Take home message: LCDD should be considered in Congo Red negative glassy eosinophilic deposits and can be highlighted by other commonly available histochemical stains.
References
Wei P, Tao R, Liu Y, et al. Pulmonary light chain deposition disease: a case series and literature review. Ann Transl Med. 2020;8(9):588. doi:10.21037/atm-20-2708
Bhargava P, Rushin JM, Rusnock EJ, et al. Pulmonary light chain deposition disease: report of five cases and review of the literature. Am J Surg Pathol. 2007;31(2):267-276. doi:10.1097/01.pas.0000213358.18380.d2
Colombat M, Holifanjaniaina S, Guillonneau F, et al. Mass spectrometry-based proteomic analysis: a good diagnostic tool for cystic lung light chain deposition disease. Am J Respir Crit Care Med. 2013;188(3):404-405. doi:10.1164/rccm.201301-0071LE
Colombat M, Stern M, Groussard O, et al. Pulmonary cystic disorder related to light chain deposition disease. Am J Respir Crit Care Med. 2006;173(7):777-780. doi:10.1164/rccm.200510-1620CR
Contributors
Assistant Professor of Pathology
Department of Pathology and Laboratory Medicine
Western University
London, Ontario, Canada