
Click here to see all images
May, 2022
Case of the Month
Clinical History: : A 55-year-old woman with past history of thymoma and papillary thyroid cancer underwent allogeneic stem cell transplantation for aplastic anemia. In the course of her illness, she developed pleural thickening/scarring with small pleural effusion. Due to its progressive nature, a clinical concern to exclude a neoplastic process was present. Hence, the patient underwent right upper lobe wedge biopsies. Figure 1 (A-D) shows coronal and axial CT images of the lung. Figures 2-4 show H&E photomicrographs and Figures 5 and 6 show the elastin van-Gieson stained photomicrographs.
Q1. Which of the following are in the differential diagnosis for a combination of both pleural and parenchymal fibrosis?
- Asbestosis
- Advanced (fibrosing) sarcoidosis
- Radiation or drug induced lung disease
- Pleuroparenchymal fibroelastosis
- All of the above
Q2. Which of the following is the best diagnosis when you encounter a combination of intra-alveolar fibrosis and septal elastosis?
- Asbestosis
- Advanced (fibrosing) sarcoidosis
- Radiation or drug induced lung disease
- Pleuroparenchymal fibroelastosis
Q3. Is this statement true or false? The localized lesion of the apices of the upper lobes, the so-called “pulmonary apical cap”, is typically asymptomatic and non-progressive compared to PPFE.
- True
- False
Answers to Quiz
Q2. D
Q3. True
Diagnosis
Discussion
In 1992, Amitani first described this pattern of idiopathic upper lobe fibrosis in the Japanese literature. Frankel et al defined a similar type of fibrotic syndrome as a “unique idiopathic pleuroparenchymal lung disease”, which was characterized by upper lobe predominance radiologically. The pathologic findings did not fit with any of the previously defined interstitial pneumonias. In 2013, this entity received formal recognition as a rare idiopathic interstitial pneumonia. The exact nature of the initiating processes remains unknown. There are idiopathic and non-idiopathic types described in the current literature. The most common setting is bone marrow/hematopoietic stem cell as well as lung transplantation. Others include chemotherapeutic agent administration, connective tissue disease, acute infective type of lung injury, chronic hypersensitivity pneumonitis (CHP) and asbestos/aluminum exposures as an occupational hazard. Clinically, this has been reported in children and elderly individuals with a bimodal age distribution from 13-85 years with a mean of 49 years.
High resolution computed tomography images (Figure 1) show coronal (A-C) and axial (B-D) lung window CT images demonstrating a progressive biapical fibrotic process with involvement of pleura and subpleural lung parenchyma. Note the pleural thickening in the right apex (red arrow) (C-D) with architectural distortion, traction bronchiectasis (curved down arrow) and volume loss. There is gradual elevation of the hila (green arrow) and the right minor fissure (yellow arrow) (C) and approximation of the trachea to the spine (D). Progression of pleural thickening and fibrosis is noted in Figure 1 (C and D), 5 years later than the initial images (A and B).
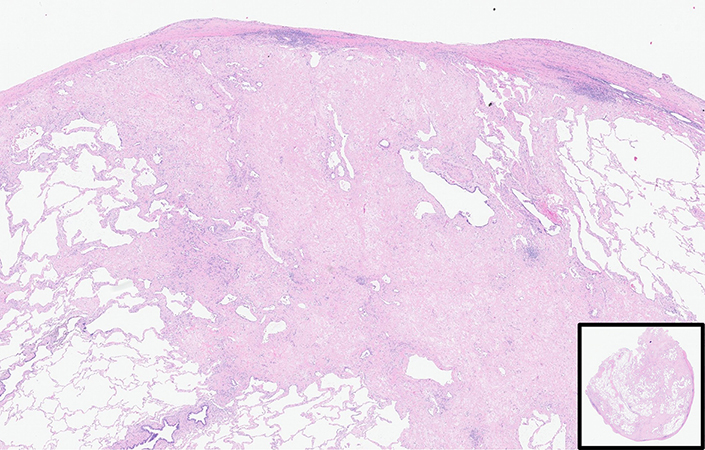
Histopathology shows upper zone pleural thickening with subpleural fibrosis with less or no lower lobe involvement. The combination of visceral pleural fibrosis and intra-alveolar fibrosis is noted in Figure 2. Although it is predominantly seen in a subpleural distribution, deeper extension is seen in Figure 2 with involvement around the bronchovascular bundles (Figure 3) and residual alveolar spaces (Figure 4). Even on the H&E slide, septal elastosis can be appreciated, but elastic van Gieson stain highlights the elastotic nature of the process (Figures 5 and 6). Usual interstitial pneumonia (UIP) may co-exist in the lower lobe as reported in the literature. Current evidence suggests that some patients with PPFE are more likely to develop progressive disease, including the idiopathic types, people with short telomere lengths and concomitant CHP or UIP. Corticosteroids and immunosuppressive agents such as methotrexate or Azathioprine are best avoided due to increase in risk of infections.
Pirfenidone is being evaluated as part of a clinical trial. Lung transplant has been the only option available in these patients with some success.
Take home message for trainees: Think of PPFE when a combination of visceral pleural fibrosis and extensive intra-alveolar septal elastosis is present.
References
2. Chua F, Desai SR, Nicholson AG et al. Pleuroparenchymal fibroelastosis. A review of clinical, radiological, and pathological characteristics. Ann Am Thorac Soc. 2019;16:1351-9.
3. Frankel SK, Cool CD, Lynch DA et al. Idiopathic pleuroparenchymal fibroelastosis: description of a novel clinicopathologic entity. Chest 2004;126:2007-13.
Contributors
Assistant Professor of Pathology
Pulmonary Pathologist
Director, Immunohistochemistry
Department of Pathology
Virginia Commonwealth University
Richmond, VA
Leila Rezai Gharai, M.D
Assistant Professor of Radiology
Division of Diagnostic Radiology
Virginia Commonwealth University
Richmond, VA