
Click here to see all images
October, 2022
Case of the Month
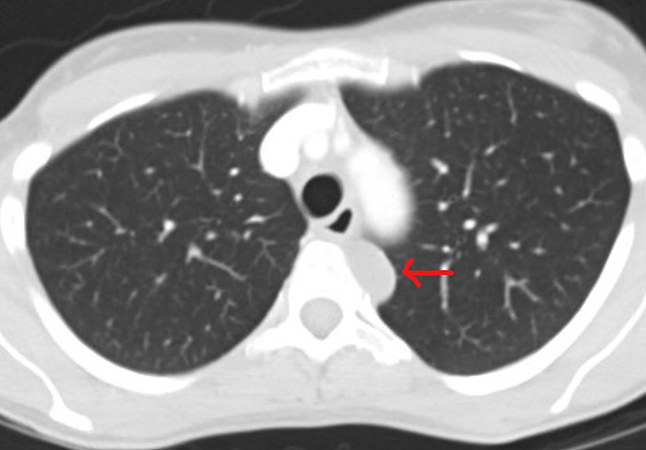
Clinical History: A 43-year-old woman was referred for a thoraco-abdomino-pelvic CT scan following mild unintentional weight loss in the context of a significant family history of colorectal cancer. There was no significant personal past medical history, and the patient was a non-smoker. Prior colonoscopy and gastroscopy were normal. The only finding on CT was 2 cm cystic lesion of the left posterior mediastinum. Follow up imaging 6 months later showed that the cyst had increased to 3 cm in size (Figure 1) and an excision was performed. Intraoperatively the lesion was extrapulmonary and adherent to the pleura of the posterior mediastinum, however the surgeon noted that complete surgical excision without rupture was achieved. Macroscopically the specimen consisted of two thin (~0.2 cm) fragments of uniform fibro-membranous tissue without excrescences or nodules, the largest of which was 2.5 cm in greatest diameter. The specimen was entirely submitted for histologic examination. Histologic sections showed relatively uniform bands of epithelial lined fibrous tissue with occasional luminal papillary-like extensions and tubular involutions (Figures 2, 3, 4). No cartilage, submucosal type glands, or thymic tissue were identified. Representative positive immunohistochemical stains are provided (Figures 5, 6).
Q1. The epithelium of this lesion would be expected to be positive for which of the following immunostains:
- CK 5/6
- PAX8
- CDX2
- D2-40
Q2. The most common thoracic location for these lesions is:
- Anterior mediastinum
- Visceral pleura
- Supradiaphragmatic
- Posterior mediastinum
Q3. Based on histologic features alone, which of the following entities would be least likely in considering the differential diagnosis for this case:
- Bronchogenic cyst
- Foregut cyst
- Thymic cyst
- Teratoma
Answers to Quiz
Q2. D
Q3. C
Diagnosis
Discussion
The presence of ciliated cells in this case helps to narrow the differential diagnosis of cystic mediastinal lesions. As there is no thymic tissue components (lymphocytes or epithelium), a thymic cyst is essentially excluded. A bronchogenic cyst should be considered, however most authors agree that either cartilage or submucosal glands are usually required to make a definitive diagnosis of this entity. In the absence of such structures, a foregut cyst (or « primitive foregut cyst ») would remain in the differential diagnosis, however these types of cysts generally contain goblet cells typical of respiratory epithelium and immunohistochemical markers of Müllerian differentiation would be absent. Since Müllerian epithelium can be a component of a mediastinal teratoma, complete sampling (and complete excision) of the lesion is important. As mature/adult-type teratomas are characterized by a haphazard admixture of multiple tissue types, the organized architecture and single tissue type in the featured case made this diagnosis less likely. Other mediastinal cysts to keep in mind but generally not associated with ciliated epithelium are esophageal duplication cyst, thoracic duct cyst, mesothelial/pericardial/celomic/serous cyst, and gastro-enteric cyst.
Take home message for trainees: Müllerian cysts should be included in the differential diagnosis when approaching a case of a mediastinal cysts with ciliated cells in a woman. .
References
Miura H, MiuraJ, Hirano H. Mediastinal cysts with mullerian differentiation. Respirol Case Rep. 2018 May 3;6(5)
Hattori H. Ciliated cyst of probable mullerian origin arising in the posterior mediastinum. Virchows Arch. 2005 Jan;446(1):82-4
Contributors
Pathologist and Associate Professor
University of Montreal Health Centre
Montreal, Canada