
Click here to see all images
September, 2022
Case of the Month
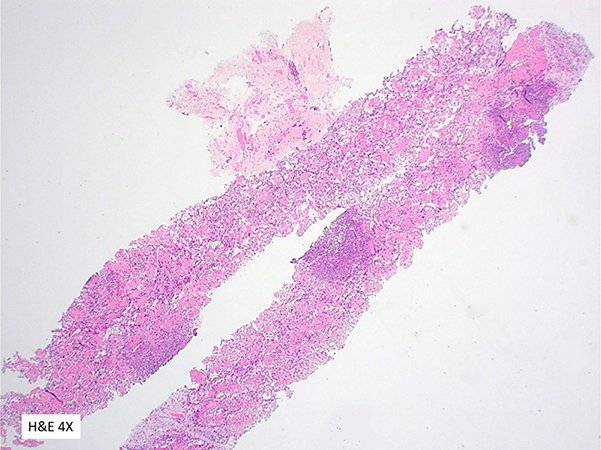
Clinical History: A 52-year-old-woman presented with cough, chest pain, and some subjective fevers. The patient had undergone cadaveric orthotopic liver transplant two years prior to presentation. A subsequent chest CT demonstrated a solid-appearing 2 cm nodule within the left upper lobe. A core needle biopsy was performed (Figures 1-6).
Q1. Which of the following is true regarding this organism?
- It is readily cultured from sputum.
- Infection is more common in immunocompetent patients.
- Hematogenous dissemination is common.
- The lung is an uncommon primary site of infection.
Q2. Which of the following is true regarding this organism?
- It is readily visualized on H&E-stained sections.
- It is tissue Gram stain negative.
- So-called ‘sulfur’ granules are a typical accompanying feature.
- They are weakly acid-fast.
Q3. Which of the following is true regarding this organism?
- Necrotizing bronchopneumonia with abscess formation is the typical histopathologic feature.
- Treatment typically involves sulfonamide therapy.
- Brain abscesses may develop if untreated or treatment is delayed.
- All of the above
Answers to Quiz
Q1. C
Q2. D
Q3. D
Q2. D
Q3. D
Diagnosis
Pulmonary nocardiosis.
Discussion
Histologic sections of the biopsy demonstrate a fibrinous-appearing pneumonia with numerous small abscess-like formations and associated necrosis. High-magnification demonstrates the fibrinous material to be vaguely filamentous in nature with some weakly basophilic-appearing strands present within the abscess-like formations on the hematoxylin and eosin (H&E)-stained slides. True granulomatous inflammation was not identified. Given the inflammatory nature of the findings, Ziehl-Neelsen (AFB) and Grocott methenamine silver stain (GMS) were initially performed. The AFB stain demonstrated small thin organisms with a beaded-appearing staining pattern. The GMS stain revealed numerous thin, branching filamentous organisms. A modified acid-fast stain (Fite) recapitulated the staining pattern seen on the GMS-stained sections.
Worldwide infection by Nocardia species depends on and varies with the type of infection. In tropical and subtropical climates cutaneous infection is most common and usually secondary to trauma. Aside from cutaneous infection, the lung is the most common primary site of infection by Nocardia and Nocardia asteroides is usually the offending species. Most patients with pulmonary nocardiosis are immunocompromised, particularly transplant patients, or have other underlying diseases that predispose them to infection, such as COPD or bronchiectasis. Clinical symptoms vary and range from mild chest complaints to fulminant toxic illness. Radiographically, findings range from solitary to diffuse nodularities or often cavitary infiltrates. Hematogenous dissemination to the brain is common and more likely to occur if untreated or therapy is delayed. Therefore, it is critical to promptly identify and treat patients with pulmonary nocardiosis. Treatment typically involves sulfonamide therapy. Organisms frequently cannot be cultured from induced sputum and biopsy is often indicated for diagnosis.
Histologically pulmonary nocardiosis is characterized by a necrotizing bronchopneumonia with abscess formation. Poorly formed granulomas may be seen in areas of necrosis. Typically, the organisms cannot be well visualized on H&E-stained sections but may be seen as weakly basophilic filaments. Organisms may also be seen faintly staining on Papanicolaou- or Diff-Quick-stained cytology preparations. The organisms are tissue Gram stain positive and are well visualized on GMS-stained sections. The bacteria are thin (usually a micron or less), branching, and filamentous. The organisms are weakly acid-fast and appear thin and beaded on AFB-stained sections, potentially raising concern for a mycobacterial infection. The acid-fast staining can be enhanced by use of a modified or partial acid-fast stain.
The primary differential diagnostic consideration is that of actinomycosis. The thin branching filaments of Nocardia and Actinomyces are indistinguishable on Gram and GMS-stained sections. Both organisms cause a similar type of suppurative inflammatory reaction. Actinomyces however is not acid-fast and typically forms large amphophilic granules termed ‘sulfur’ granules. These granules are usually coated by eosinophilic projections of Splendore-Hoeppli material. Differentiation and species confirmation can also be performed by molecular analyses such as 16S rRNA sequencing, as was the case for this biopsy.
Take home message for trainees: Special stains should always be considered in cases of inflammatory lung disease involving an immunocompromised patient. .
Worldwide infection by Nocardia species depends on and varies with the type of infection. In tropical and subtropical climates cutaneous infection is most common and usually secondary to trauma. Aside from cutaneous infection, the lung is the most common primary site of infection by Nocardia and Nocardia asteroides is usually the offending species. Most patients with pulmonary nocardiosis are immunocompromised, particularly transplant patients, or have other underlying diseases that predispose them to infection, such as COPD or bronchiectasis. Clinical symptoms vary and range from mild chest complaints to fulminant toxic illness. Radiographically, findings range from solitary to diffuse nodularities or often cavitary infiltrates. Hematogenous dissemination to the brain is common and more likely to occur if untreated or therapy is delayed. Therefore, it is critical to promptly identify and treat patients with pulmonary nocardiosis. Treatment typically involves sulfonamide therapy. Organisms frequently cannot be cultured from induced sputum and biopsy is often indicated for diagnosis.
Histologically pulmonary nocardiosis is characterized by a necrotizing bronchopneumonia with abscess formation. Poorly formed granulomas may be seen in areas of necrosis. Typically, the organisms cannot be well visualized on H&E-stained sections but may be seen as weakly basophilic filaments. Organisms may also be seen faintly staining on Papanicolaou- or Diff-Quick-stained cytology preparations. The organisms are tissue Gram stain positive and are well visualized on GMS-stained sections. The bacteria are thin (usually a micron or less), branching, and filamentous. The organisms are weakly acid-fast and appear thin and beaded on AFB-stained sections, potentially raising concern for a mycobacterial infection. The acid-fast staining can be enhanced by use of a modified or partial acid-fast stain.
The primary differential diagnostic consideration is that of actinomycosis. The thin branching filaments of Nocardia and Actinomyces are indistinguishable on Gram and GMS-stained sections. Both organisms cause a similar type of suppurative inflammatory reaction. Actinomyces however is not acid-fast and typically forms large amphophilic granules termed ‘sulfur’ granules. These granules are usually coated by eosinophilic projections of Splendore-Hoeppli material. Differentiation and species confirmation can also be performed by molecular analyses such as 16S rRNA sequencing, as was the case for this biopsy.
Take home message for trainees: Special stains should always be considered in cases of inflammatory lung disease involving an immunocompromised patient. .
References
Ott SR et al. Pulmonary nocardiosis in Western Europe-Clinical evaluation of 43 patients and population-based estimates of hospitalization rates. Int J Infect Dis. 2019 Apr;81:140-148.
Katzenstein AL. Diagnostic Atlas of Non-Neoplastic Lung Disease: A practical guide for surgical pathologist.
Procop GW, Pritt BS. Foundations in Diagnostic Pathology: Pathology of Infectious Disease. .
Katzenstein AL. Diagnostic Atlas of Non-Neoplastic Lung Disease: A practical guide for surgical pathologist.
Procop GW, Pritt BS. Foundations in Diagnostic Pathology: Pathology of Infectious Disease. .
Contributors
Scott W. Aesif, M.D., Ph.D.
Senior Associate Consultant
Mayo Clinic Florida
Jacksonville, Florida
Senior Associate Consultant
Mayo Clinic Florida
Jacksonville, Florida