
Click here to see all images
February, 2023
Case of the Month
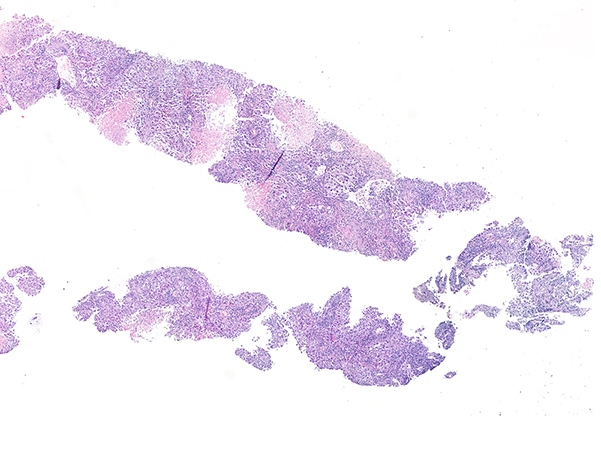
Clinical History: An 87-year-old male never smoker with multiple resected meningiomas presented with dyspnea. His CT shows multiple bilateral pulmonary nodules, with a dominant mass measuring 36 mm in the right upper lobe and mediastinal lymphadenopathies. No other history of cancer was known. A percutaneous lung biopsy was performed. Histological sections are shown in figures 1 and 2. Figure 3 corresponds to TTF1 (8G7G3/1) and figure 4 to p40.
Q1. Which of these statements is false?
- 8G7G3/1 is a highly specific clone of TTF1.
- TTF1 is staining non-neoplastic pneumocytes.
- TTF1 is negative in almost 20% of adenocarcinomas. Morphology is enough in this case for diagnosing adenocarcinoma.
- TTF1 and p40 are both negative, morphology suggests carcinoma but is not conclusive. Revision of clinical history and additional IHC markers are recommended.
Q2. CK AE1/AE3 staining was performed, and it was negative. Which of the following should be considered in an expanded differential diagnosis?
- Melanoma
- SMARCA4 undifferentiated tumor
- Large cell undifferentiated carcinoma
- All the above
Q3. In addition to melanoma which of the following tumors is Sox10 often positive?
- Adenoid cystic carcinoma
- Basaloid squamous cell carcinoma
- Metaplastic breast cancer
- All the above
Answers to Quiz
Q1. C
Q2. D
Q3. D
Q2. D
Q3. D
Diagnosis
Melanoma
Discussion
In lung diagnostic samples, the amount of tissue is limited, and it needs to be used for accurate histological classification and, in many cases for biomarker testing. Well differentiated tumors with clear squamous or glandular differentiation do not require immunohistochemistry and a limited immunopanel of TTF1/p40 is sufficient in most cases to classify poorly differentiated tumors. Using this simple panel, cases that are positive for TTF-1 alone can be classified as non-small cell lung carcinoma (NSCLC) favor adenocarcinoma and p40 positive cases can be classified as NSCLC favor squamous cell carcinoma. Tumors that are negative for both TTF-1 and p40 can be reported as NSCLC not otherwise specified in a small biopsy. However, in this scenario, it is critical to consider an expanded differential diagnosis that should include metastasis from elsewhere, melanoma, sarcoma, lymphoma and other undifferentiated neoplasms. This requires reviewing the medical record and expanding the immunopanel. A diffusely positive keratin for example is enough to confirm the epithelial nature of the neoplasm.
From all the diagnostic possibilities it is important to always keep in mind melanoma because metastatic melanoma can have multiple clinical presentations. This famous mimicker can have multiple appearances from spindled to epithelioid with carcinoma-like morphology. There are also cases in which melanoma can have a lepidic growth architecture and extend along intact alveolar spaces. Some clues should make us suspect it: big nucleoli, rhabdoid features or cells infiltrating the interstitium in otherwise conventional “lepidic” neoplasm. But these features may lack like in our case.
S100 and Sox10 are the most sensitive markers for melanoma, but it is important to remember they are not specific. Sox10 can stain a subset of carcinoma including salivary, basaloid squamous cell carcinoma and metaplastic breast carcinoma. The addition of other markers such as Melan-A, and HMB45 are typically recommended to further support the classification as a melanoma.
Primary lung melanoma is a controversial entity because melanocytes are not normally found in lung. As cutaneous melanoma can undergo complete regression, it has been postulated that ‘primary’ lung melanomas represent metastasis from unrecognized or regressed skin melanomas. This hypothesis is supported by data from a recent study of patients with lung-only melanoma, which showed that all cases had a dominant ultraviolet (UV) light mutation signature on next-generation sequencing. This makes a strong argument that all melanomas in the lung are likely metastatic from non-lung sites.
Take home message for trainees: Melanoma is the great mimicker, and it is important to consider an expanded differential in tumors that are negative for p40/TTF-1. The lung is a common site for metastases from a wide spectrum of primary malignant tumors from different lineages, including sarcomas, carcinomas, and melanoma.
From all the diagnostic possibilities it is important to always keep in mind melanoma because metastatic melanoma can have multiple clinical presentations. This famous mimicker can have multiple appearances from spindled to epithelioid with carcinoma-like morphology. There are also cases in which melanoma can have a lepidic growth architecture and extend along intact alveolar spaces. Some clues should make us suspect it: big nucleoli, rhabdoid features or cells infiltrating the interstitium in otherwise conventional “lepidic” neoplasm. But these features may lack like in our case.
S100 and Sox10 are the most sensitive markers for melanoma, but it is important to remember they are not specific. Sox10 can stain a subset of carcinoma including salivary, basaloid squamous cell carcinoma and metaplastic breast carcinoma. The addition of other markers such as Melan-A, and HMB45 are typically recommended to further support the classification as a melanoma.
Primary lung melanoma is a controversial entity because melanocytes are not normally found in lung. As cutaneous melanoma can undergo complete regression, it has been postulated that ‘primary’ lung melanomas represent metastasis from unrecognized or regressed skin melanomas. This hypothesis is supported by data from a recent study of patients with lung-only melanoma, which showed that all cases had a dominant ultraviolet (UV) light mutation signature on next-generation sequencing. This makes a strong argument that all melanomas in the lung are likely metastatic from non-lung sites.
Take home message for trainees: Melanoma is the great mimicker, and it is important to consider an expanded differential in tumors that are negative for p40/TTF-1. The lung is a common site for metastases from a wide spectrum of primary malignant tumors from different lineages, including sarcomas, carcinomas, and melanoma.
References
Thoracic tumours. WHO classification of tumours series, 5th ed 2021; 5.
Rooper LM et al. SOX10 immunoexpression in basaloid squamous cell carcinomas: a diagnostic pitfall for ruling out salivary differentiation. Head Neck Pathol 2019; 13, 543-547.
Yatabe et al. Best practices recommendations for diagnostic immunohistochemistry in lung cancer. Journal of Thoracic Oncology: Official Publication of the International Association for the Study of Lung Cancer 2019; 14, 377–407.
Yang et al. Lung-only melanoma: UV mutational signature supports origin from occult cutaneous primaries and argues against the concept of primary pulmonary melanoma. Modern Pathology 2020; 33, 2244-2255.
Mukhopadhyay S, Cecchini M. Survival Guide to Thoracic Pathology. Innovative Science Press 2023; 46.
Rooper LM et al. SOX10 immunoexpression in basaloid squamous cell carcinomas: a diagnostic pitfall for ruling out salivary differentiation. Head Neck Pathol 2019; 13, 543-547.
Yatabe et al. Best practices recommendations for diagnostic immunohistochemistry in lung cancer. Journal of Thoracic Oncology: Official Publication of the International Association for the Study of Lung Cancer 2019; 14, 377–407.
Yang et al. Lung-only melanoma: UV mutational signature supports origin from occult cutaneous primaries and argues against the concept of primary pulmonary melanoma. Modern Pathology 2020; 33, 2244-2255.
Mukhopadhyay S, Cecchini M. Survival Guide to Thoracic Pathology. Innovative Science Press 2023; 46.
Contributors
Irene Sansano, MD, PhD
Staff pathologist
Department of Pathology
HU Vall d’Hebron, Barcelona, Spain
Julio Chabla, MD
Second year resident
Department of Pathology
HU Vall d’Hebron, Barcelona, Spain
Berta Ferrer, MD
Staff pathologist
Department of Pathology
HU Vall d’Hebron, Barcelona, Spain
Staff pathologist
Department of Pathology
HU Vall d’Hebron, Barcelona, Spain
Julio Chabla, MD
Second year resident
Department of Pathology
HU Vall d’Hebron, Barcelona, Spain
Berta Ferrer, MD
Staff pathologist
Department of Pathology
HU Vall d’Hebron, Barcelona, Spain