
Click here to see all images
May, 2023
Case of the Month
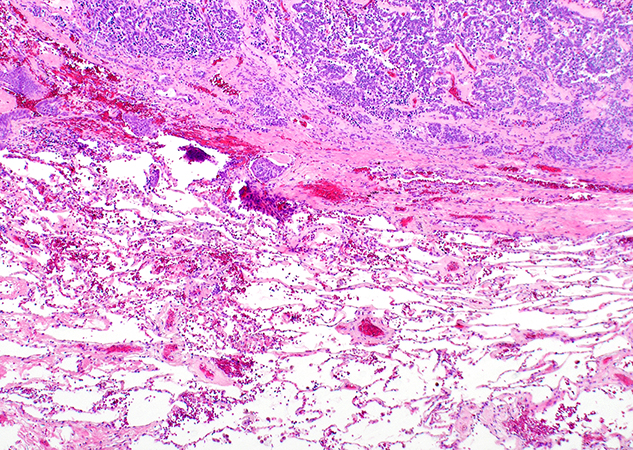
Clinical History: A 73-year-old woman with prior history of invasive ductal breast carcinoma status-post surgical resection, radiation, and endocrine therapy presented to her physician with lingering cough after COVID-19 infection. A CT scan detected a 1.8 cm indeterminate nodule in the left upper lobe with relatively smooth margins. PET/CT scan showed that the nodule was hypermetabolic with FDG avidity similar to that of the liver, suspicious for metastatic disease. The patient underwent a core biopsy of the nodule (not shown) and later left upper lobectomy. Histologic sections of the nodule are shown in Figures 1 through 6. A Fontana-Masson stain is shown in Figure 5.
Q1. What is the brown pigment present in some of the tumor cells?
- Hemosiderin
- Lipofuscin
- Melanin
- Serotonin
Q2.What is the most important diagnosis of exclusion of this lesion?
- Pulmonary thymoma
- Solitary fibrous tumor
- Spindle cell carcinoma
- Primary lung or metastatic spindle cell melanoma.
Q3. Which of the following statements is TRUE:
- The non-pigmented tumor cells are positive for HMB-45 and SOX10
- The non-pigmented tumor cells are positive for synaptophysin and chromogranin
- The Fontana-Masson stain highlights the presence of hemosiderin
- Pigmented cells are a common feature in this tumor
Answers to Quiz
Q2. D
Q3. B
Diagnosis
Discussion
The presence of uncommon morphologic features in neuroendocrine tumors can create diagnostic confusion. Evaluation of a cellular spindle cell neoplasm with scattered pigment in the lung may be confused with spindle cell melanoma (either primary or metastatic). The lack of a prior history of melanoma does not favor metastatic disease, and the bland cytologic features would be uncommon in melanoma. Pulmonary spindle cell neuroendocrine tumors should also be distinguished from pulmonary thymoma, spindle cell carcinomas, solitary fibrous tumor, and synovial sarcoma. Immunohistochemistry is helpful to establish the diagnosis of a neuroendocrine tumor, positive for CD56, synaptophysin, chromogranin and INSM1 in most cases. In the current case, neuroendocrine differentiation was confirmed in the core biopsy (not shown). Melanocytic markers (S100, HMB-45, MART-1, SOX10) are expressed only in cells containing melanin, but they are negative in the non-pigmented neoplastic neuroendocrine cells. Neuroendocrine tumors are negative for CD34, STAT6 (positive in solitary fibrous tumor), TLE1 (positive in synovial sarcoma) and p40 (positive in thymoma). Spindle cell carcinomas have significant atypia, are positive for keratins, but are negative for neuroendocrine markers. None of these tumors contain melanin.
Pigmented neuroendocrine tumors are not exclusive of the lung, with some descriptions in the thymus and the gastrointestinal tract. It is hypothesized that along with hormone production, melanin may be produced by neuroendocrine cells due to a divergent differentiation.
Most pigmented neuroendocrine tumors reported have been typical carcinoids, and only rarely atypical carcinoids. The identification of melanin in a pulmonary neuroendocrine tumor does not confer any prognosis. A pigmented neuroendocrine tumor should be graded using conventional diagnostic criteria, as done in the current case.
Take home message for trainees: Rarely, carcinoid tumors can contain melanin creating diagnostic confusion. The most important diagnosis of exclusion is spindle cell melanoma (primary or metastatic to lung). Clinical history, morphology, special stains, and immunohistochemical stains are useful to confirm the diagnosis. Identification of melanin does not confer any prognosis to a lung neuroendocrine tumor, which should be graded according to conventional WHO criteria.
References
Gal AA, Koss MN, Hochholzer L, et al. Pigmented pulmonary carcinoid tumor. An immunohistochemical and ultrastructural study. Arch Pathol Lab Med 1993;117:832-6.
Fukuda T, Kobayashi H, Kamishima T, et al. Peripheral carcinoid tumor of the lung with focal melanin production. Pathol Int 1994;44:309-16.
Goel A, Addis BJ. Pigmented atypical carcinoid of the lung. Histopathology 2007;51:263-5.
Contributors
First year resident
Department of Pathology
Duke University Medical Center
Durham, NC
Sergio Pina-Oviedo, MD
Assistant Professor
Department of Pathology
Duke University Medical Center
Durham, NC
Elizabeth Pavlisko, MD
Associate Professor
Department of Pathology
Duke University Medical Center
Durham, NC
Carolyn Glass, MD, PhD
Associate Professor Department of Pathology
Duke University Medical Center
Durham, NC
Thomas Sporn, MD
Professor
Department of Pathology
Duke University Medical Center
Durham, NC
Victor Roggli, MD
Professor
Department of Pathology
Duke University Medical Center
Durham, NC