
Click here to see all images
October, 2023
Case of the Month
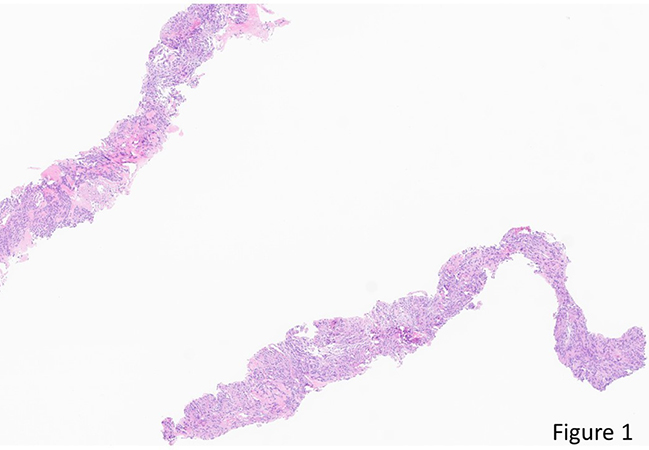
Clinical History: A 70-year-old man with an apparently isolated lower lobe lung mass underwent CT-guided core needle biopsy. On H&E sections (Figure 1: 40x, Figure 2: 200x, Figure 3: 400x) there are up to 4 mitotic figures per 3 high-power fields. The neoplasm has patchy reactivity with antibodies directed against EMA (Figure 4) and progesterone receptor (Figure 5), and diffuse strong reactivity with antibodies directed against SSTR2A (Figure 6). There is no reactivity with antibodies directed against AE1/AE3, TTF-1, napsin A, p40, synaptophysin, SOX10, S100, STAT6 or CD34.
Q1. The morphologic differential diagnosis for the H&E appearance of this spindle cell neoplasm includes
- Metastatic thymoma
- Solitary fibrous tumor
- Monophasic synovial sarcoma
- All of the above
Q2. Which of the following features would NOT support a diagnosis of pulmonary meningioma?
- Size usuall > 4 mm
- Irregular borders
- Transitional or fibrous patterns
- Psammoma bodies
Q3. Pulmonary meningiomas are typically positive for which of the following immunostains:
- SSTR2A
- Sox1
- Synaptophysin
- Pankeratin
Answers to Quiz
Q2. B
Q3. A
Diagnosis
Discussion
Like their CNS counterparts, pulmonary meningiomas are often positive for EMA and progesterone receptor. Immunohistochemistry for somatostatin receptor 2A (SSTR2A) shows diffuse and strong staining in almost all CNS meningiomas, as well as in pulmonary meningiomas, but is also positive in some neuroendocrine neoplasms, gastrointestinal stromal tumors and follicular dendritic cell sarcomas. Occasional cases of pulmonary meningioma have shown CD56, CD34, S100, smooth muscle actin, calretinin or CD117 immunoreactivity. Other melanoma markers, neuroendocrine markers and cytokeratins are expected to be negative, although cytokeratin expression has been noted in malignant CNS meningiomas. Mutations in NF2, BAP1 and other genes have been identified CNS meningiomas, but the frequency of these alterations in pulmonary meningiomas remains unclear.
There are multiple theories as to the origin of pulmonary meningioma, including possible origin from heterotopic rests, pluripotent stem cells, or meningothelioid nodules. Although cases with co-occurrence of meningothelioid nodules and meningioma have been reported, molecular features of meningioma and meningothelioid nodules appear distinct. Morphologically, meningioma and meningothelioid nodules may be distinguished by their location, circumscription and size: meningothelioid nodules tend to be interstitial and perivenular, have irregular, ill-defined borders and are typically ≤3 mm in size, whereas meningiomas are well-circumscrib
Take home message
Consider meningioma in the differential diagnosis for a spindle cell neoplasm of the lung.
References
Ionescu DN, Sasatomi E, Aldeeb D, et al. Pulmonary meningothelial-like nodules: a genotypic comparison with meningiomas. Am J Surg Pathol 2004;28:207-214. Liu X, Xu X, Zou Y.
Pulmonary primary meningioma: A report of two cases and review of the literature. Heliyon 2023;9:e16705.
Motoi N, Duhig EE. Meningioma of the lung. In: WHO Classification of Tumours Editorial Board. Thoracic tumours. Lyon (France): International Agency for Research on Cancer; 2021. (WHO classification of tumours series, 5th ed.; vol. 5). https://publications.iarc.fr/595.
Sahm F, Perry A, von Deimling A, et al. Meningioma. In: WHO Classification of Tumours Editorial Board. Central nervous system tumours. Lyon (France): International Agency for Research on Cancer; 2021. (WHO classification of tumours series, 5th ed.; vol. 6). https://publications.iarc.fr/601.
Contributors
Consultant Pathologist
Vancouver General Hospital
Vancouver, BC, Canada
Dr. Joseph Maleszewski
Consultant Pathologist
Mayo Clinic
Rochester MN
USA