
Click here to see all images
February, 2024
Case of the Month
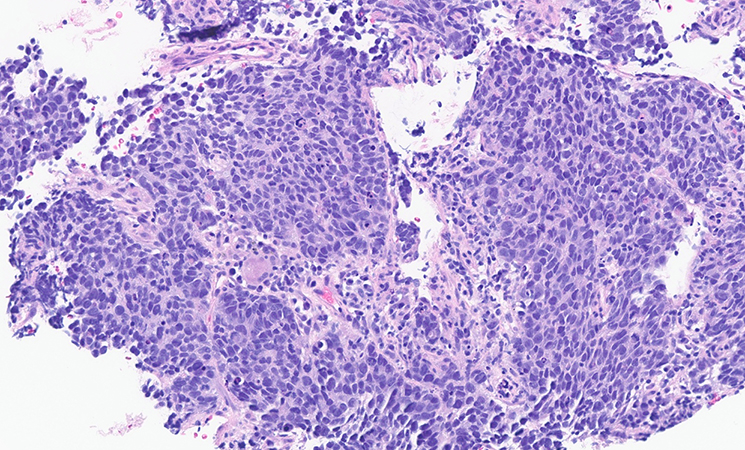
Clinical History: An 84-year-old woman with a history of smoking was found to have a 7.6 cm mass in the right lower lobe with satelite lesions and FDG-avid thoracic lymphadenopathy. Endobronchial ultrasound sampling of the 4R lymph node showed an abnormal population of small to intermediate-sized cells arranged in solid nests and rosettes with prominent crush artifact (Figure 1). The cells show high nuclear to cytoplasmic ratios, nuclear molding, scant cytoplasm, and fine chromatin with occasional indistinct nucleoli (Figure 2). Mitotic forms and apoptotic forms are easily identified. Work-up demonstrates diffuse keratin AE1/AE3 expression (Figure 3), whilst antibodies directed against synaptophysin, chromogranin, INSM1, p40, desmin, MyoD1, and TTF-1 (Figure 4) are non-reactive. There is focal membranous staining for CD56 (Figure 5). POU2F3 is positive (Figure 6). Ki-67 is over 90%.
Q1. What is the most likely diagnosis?
- Small cell carcinoma
- Adenocarcinoma
- Carcinoid tumor
- Sarcoma
Q2. What is the useful IHC marker for making the diagnosis of neuroendocrine-negative SCLC?
- ASCL1
- NEUROD1
- POU2F3
- BAP1
Q3. POU2F3 is a master transcriptional regulator of what kind of cells?
- Pneumocytes
- Monocytes
- Neuroendocrine cells
- Tuft cells
Answers to Quiz
Q2. C
Q3. D
Diagnosis
Discussion
Histologically, SCLC is characterized by small to intermediate sized cells with high N:C ratios, salt-and-pepper or smudgy chromatin, indistinct or absent nucleoli, nuclear molding, punctate necrosis, abundant mitosis, and cellular fragility that may classically manifest in the so-called ‘Azzopardi effect’ (encrustation of nuclear DNA around blood vessels). Architectural patterns include many that are typical to neuroendocrine-family tumors including solid, trabecular, rosettes, and spindled forms. By definition, SCLC requires > 10 mitoses/2 mm2, and a minority of cases are combined with NSCLC or with large cell neuroendocrine carcinoma.
The differential diagnosis includes other small round blue cell tumors, including basaloid squamous cell carcinoma, lymphoma, atypical carcinoid tumors, as well as various sarcomas. As these may be morphologically indistinct, immunohistochemical confirmation is usually prudent to ensure proper patient management. The majority of SCLC stain positively with keratin, TTF-1, and neuroendocrine markers. However, approximately 10% of SCLC may be negative for TTF-1 as well as negative for the most widely used neuroendocrine markers chromogranin and synaptophysin, with a smaller percentage without appreciable CD56 expression. The TTF-1 negative tumors tend to be those with low or absent neuroendocrine marker expression, and can pose diagnostic challenges.
Genomically, most SCLC is characterized by inactivating RB1 and TP53 alterations, but recent epigenetic and gene expression studies have revealed disease heterogeneity in transcription factor expression patterns, yielding four main subtypes of SCLC: SCLC-A (ASCL1-high), SCLC-N (NeuroD1-high), SCLC-P (POU2F3-high), and SCLC-Y (YAP1-high)/triple negative/inflamed.
POU2F3 (POU class 2 homeobox 3; also known as SKN-1a/OCT-11) is a transcription factor required for the generation of chemosensory cells - “tuft cells” - that are found in mucosal surfaces throughout the body, thought to be involved in immunomodulatory functions. Expression of POU2F3 was first described in SCLC by Huang et al. who determined that this subset of SCLC (SCLC-P) was associated with low neuroendocrine expression. Subsequent studies have further characterized the transcriptomic and epigenetic profile of SCLC-P, with POU2F3 expression found to be mutually exclusive of other SCLC transcriptional subtype markers ASCL1, NEUROD1, and YAP1. A study by Baine et al. showed that POU2F3 was expressed in 75% (15 of 20 cases) of SCLC with minimal to no neuroendocrine marker expression, proving its utility in supporting a diagnosis of SCLC in this context, as in this case.
It is important to note that POU2F3 expression is by no means specific to SCLC. As tuft cells are distributed throughout the body, POU2F3 may be expressed diffusely in various carcinomas, including thymic, colorectal, and breast primaries amongst others. Currently, the POU2F3 expression holds no prognostic or clinical value. However, as more clinical studies characterize the ‘tuft cell’ subset of SCLC as well as other POU2F3 related malignancies, it may one day become an actionable, clinically relevant, and druggable target.
References
Baine MK, Febres-Aldana CA, Chang JC, et al. POU2F3 in SCLC: Clinicopathologic and Genomic Analysis With a Focus on Its Diagnostic Utility in Neuroendocrine-Low SCLC. J Thorac Oncol 2022;17: 1109-1121.
D'Angelo E, Pastrello C, Biccari A, et al. An integrated multiomics analysis of rectal cancer patients identified POU2F3 as a putative druggable target and entinostat as a cytotoxic enhancer of 5-fluorouracil. Int J Cancer 2023;153: 437-449.
Gay CM, Stewart CA, Park EM, et al. Patterns of transcription factor programs and immune pathway activation define four major subtypes of SCLC with distinct therapeutic vulnerabilities. Cancer Cell 2021;39: 346-360.e7.
Huang YH, Klingbeil O, He XY, et al. POU2F3 is a master regulator of a tuft cell-like variant of small cell lung cancer. Genes Dev 2018;32: 915-928.
Owonikoko TK, Dwivedi B, Chen Z, et al. YAP1 Expression in SCLC Defines a Distinct Subtype With T-cell-Inflamed Phenotype. J Thorac Oncol 2021;16: 464-476.
Rudin CM, Poirier JT, Byers LA, et al. Molecular subtypes of small cell lung cancer: a synthesis of human and mouse model data. Nat Rev Cancer 2019;19: 289-297.
Schneider C, O’Leary CE, Locksley RM. Regulation of immune responses by tuft cells. Nat Rev Immunol 2019;19: 584-593.
Yamada Y, Simon R, Iwane K, et al. An exploratory study for tuft cells in the breast and their relevance in triple-negative breast cancer: the possible relationship of SOX9. BMC Cancer 2023;23: 438.
Yamada Y, Sugimoto A, Hoki M, et al. POU2F3 beyond thymic carcinomas: expression across the spectrum of thymomas hints to medullary differentiation in type A thymoma. Virchows Arch 2022; 480: 843-851.
Contributors
Ariel Sandhu M.B., B.Ch. BAO
Pulmonary Pathology Fellow
Mayo Clinic, Rochester, MN
Ying-Chun Lo, M.D., Ph.D.
Consultant, Divisions of Anatomic Pathology and Laboratory Genetics and Genomics, Department of Laboratory Medicine and Pathology
Mayo Clinic, Rochester, MN