
Click here to see all images
January, 2024
Case of the Month
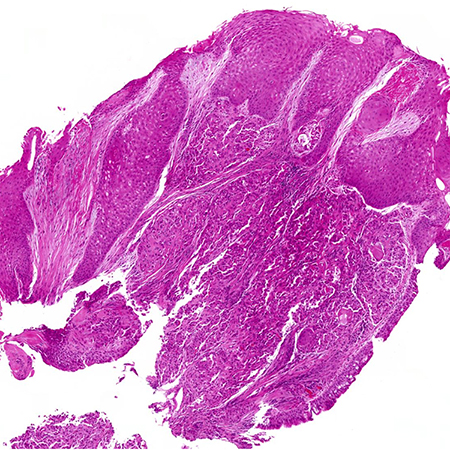
Clinical History: A pediatric patient presented with a suspected febrile illness and underwent antibiotic treatment. A chest x-ray revealed a collapse of the left lower lung lobe. Although an aspirated foreign body was initially suspected in this age group, none was detected on the x-ray or subsequent CT scan. The CT scan revealed an obstructive lesion at the lower lobe bronchus. Bronchoscopy identified a mass at the entrance of the inferior segment, causing complete collapse of the lower lobe. The initial biopsy showed lobular proliferation of cuboidal epithelial cells within a fibrovascular stroma. These cells, illustrated in figures 1 and 2, displayed monomorphic oval nuclei with minimal nuclear atypia, abundant eosinophilic cytoplasm that was focally clear and granular. No mitotic figures or necrosis were observed. Immunohistochemical analysis showed the cells were pan-cytokeratin positive and negative for TTF1, p40, CD68, ERG, synaptophysin, chromogranin, CD56, SOX10, CD117, p63, mammaglobin, and DOG1. A preliminary diagnosis of low-grade epithelial neoplasm was established, and further molecular testing revealed MAML2 rearrangement by break apart FISH (figure 3).
Q1. What is the most likely diagnosis based on the morphology and MAML2 rearrangement by FISH?
- Adenocarcinoma
- Mucoepidermoid carcinoma
- Carcinoid tumor
- Adenoid cystic carcinoma
Q2. Which three cell types are typically observed in Mucoepidermoid Carcinoma?
- Eosinophilic, mucinous, clear
- Glandular, indeterminate, clear
- Squamoid, glandular (mucinous), and intermediate
- Basaloid, squamous, keratinizing
Q3. What is the most common malignant tracheobronchial and parenchymal tumor in children?
- Carcinoid / pleuropulmonary blastoma
- Squamous cell carcinoma / adenocarcinoma
- Mucoepidermoid carcinoma / pleuropulmonary blastoma
- Carcinoid / adenocarcinoma
Q4. Which fusions are associated with mucoepidermoid carcinoma?
- CRTC1::MAML2
- CRCTC2::MAML2
- MAML2::CEP126
- All of the above
Answers to Quiz
Q2. C
Q3. A
Q4. D
Diagnosis
Discussion
The subsequent lobectomy revealed a 3.0 cm obstructing tumor (figure 4) with similar histology (figure 5) and immunoprofile (positive for pan-cytokeratin and cytokeratin 7, negative for p40, S100, and SOX10) to the biopsy. Mucicarmine stain demonstrated intracytoplasmic mucin in some cells (figure 6). Lung mucoepidermoid carcinomas are graded on cystic growth pattern, cytologic atypia, and necrosis. This case's cytomorphology aligned with low-grade mucoepidermoid carcinoma.
Differentiating high-grade mucoepidermoid carcinoma from adenosquamous carcinoma in adults can be challenging. The presence of keratinization strongly suggests squamous cell carcinoma, as individual cell keratinization or squamous pearl formation is not typically seen in mucoepidermoid carcinoma. Characteristics supporting mucoepidermoid carcinoma over adenosquamous include a proximal exophytic endobronchial location, transition from low- to high-grade histology, absence of overlying squamous cell carcinoma in situ, and lack of tubular, papillary, acinar, and papillary growth patterns.
Complete excision of the tumor is associated with an excellent prognosis for low-grade mucoepidermoid carcinomas. High-grade tumors carry a prognosis akin to other non-small cell carcinomas. Incomplete resection and nodal metastases are indicators of poor prognosis.
Take home message for trainees:
Mucoepidermoid carcinoma are rare malignant neoplasms that can occur in pediatric populations. Recent studies have expanded this diagnostic entity to include lesions without squamous differentiation based on the presence of characteristic MAML2 fusions.
References
Bishop JA, Thompson LDR, Siegele B, Gagan J, Mansour M, Chernock RD, Rooper LM. Mucoepidermoid carcinoma may be devoid of squamoid cells by immunohistochemistry: expanding the histologic and immunohistochemical spectrum of MAML2- rearranged salivary gland tumours. Histopathology. 2023 Jan;82(2):305-313. doi: 10.1111/his.14817. Epub 2022 Oct 28. PMID: 36208053.
Salem A, Bell D, Sepesi B, Papadimitrakopoulou V, El-Naggar A, Moran CA, Kalhor N. Clinicopathologic and genetic features of primary bronchopulmonary mucoepidermoid carcinoma: the MD Anderson Cancer Center experience and comprehensive review of the literature. Virchows Arch. 2017 Jun;470(6):619-626. doi: 10.1007/s00428-017-2104-4. Epub 2017 Mar 25. PMID: 28343305.
Yousem SA, Hochholzer L. Mucoepidermoid tumors of the lung. Cancer. 1987 Sep 15;60(6):1346-52. doi: 10.1002/1097-0142(19870915)60:6<1346::aid-cncr2820600631>3.0.co;2-0. PMID: 3040215.
Molina JR, Aubry MC, Lewis JE, Wampfler JA, Williams BA, Midthun DE, Yang P, Cassivi SD. Primary salivary gland-type lung cancer: spectrum of clinical presentation, histopathologic and prognostic factors. Cancer. 2007 Nov 15;110(10):2253-9. doi: 10.1002/cncr.23048. PMID: 17918258.
Contributors
Assistant Professor of Pathology
Department of Pathology and Laboratory Medicine
Western University
London, Ontario, Canada